Ultrasound examination
Examination Protocol
Ventral view
- Transverse plane
- Inclined plane
Medial view
- Transverse plane
- Inclined plane
Lateral view
- Transverse plane
- Inclined plane
Dorsal view
- Transverse plane
- Sagittal plane
Interactive feature, available in the app
1. Ventral view
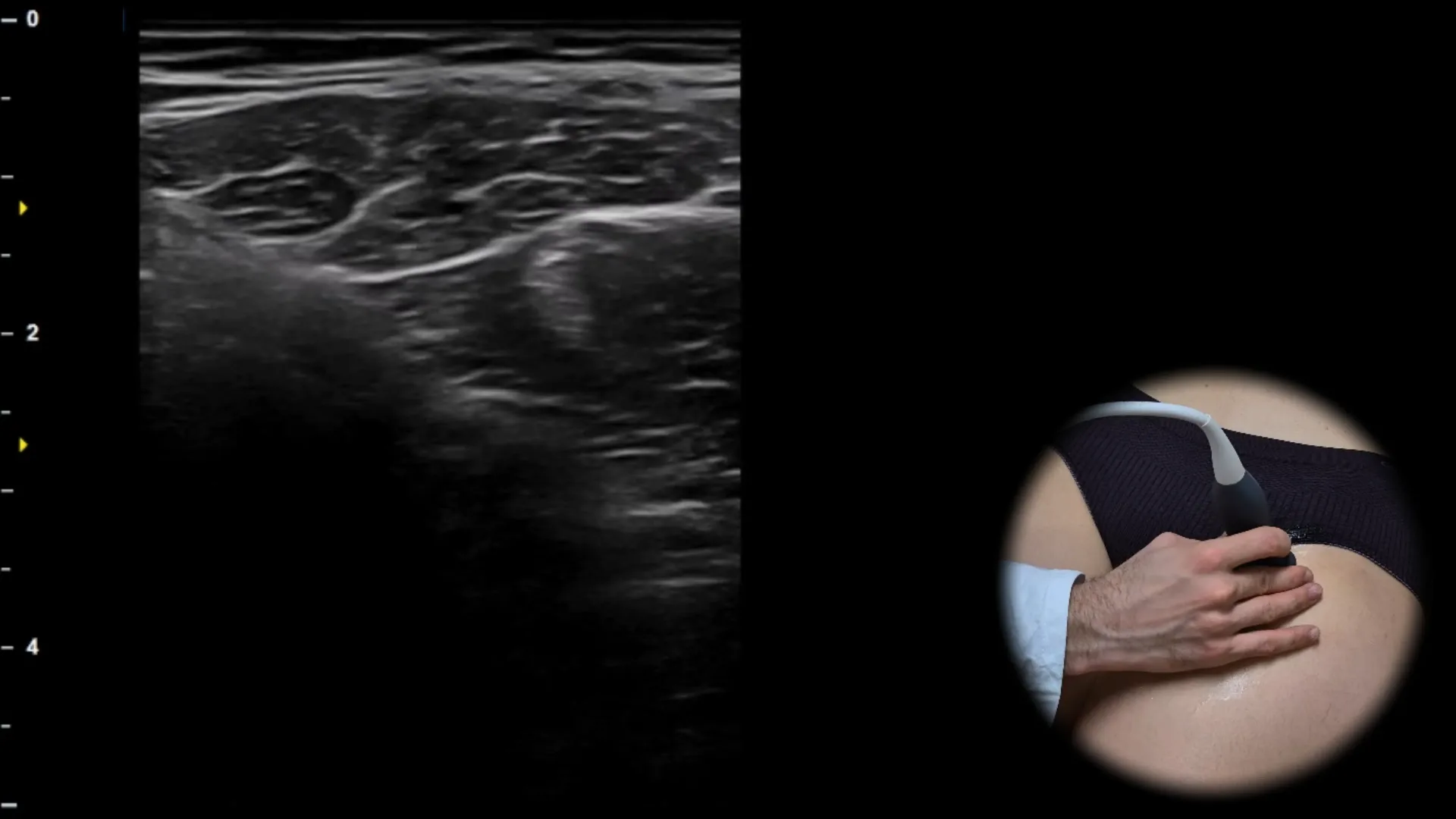
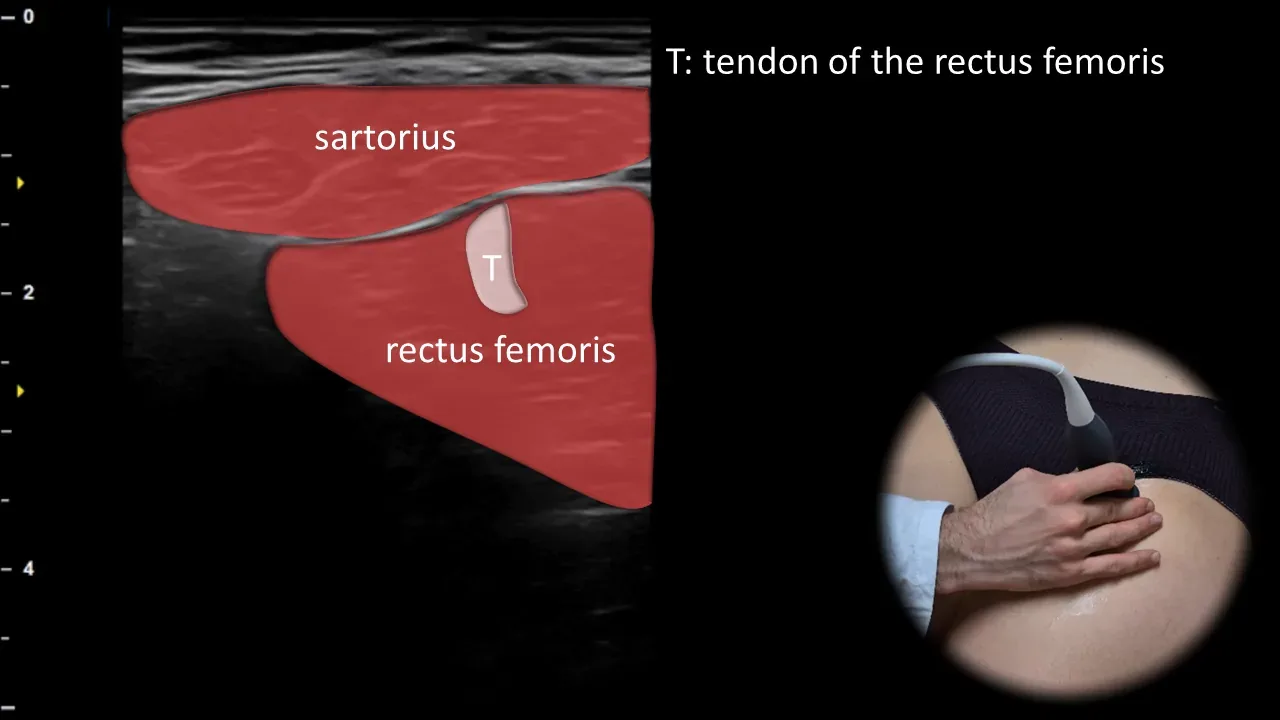
Figure 1. Ventral view, transverse plane. T: rectus femoris tendon
Transverse ultrasound section of the anterior thigh showing the superficially located sartorius muscle, running obliquely from lateral to medial, and the deeper rectus femoris muscle. Within its muscle belly, the central tendon (T) is visible, which appears as a hyperechoic linear structure and becomes more clearly demarcated in its deeper course toward the insertion. This projection is important for evaluating the myotendinous junction of the rectus femoris and for detecting muscle overuse, strain, or tendinopathy.
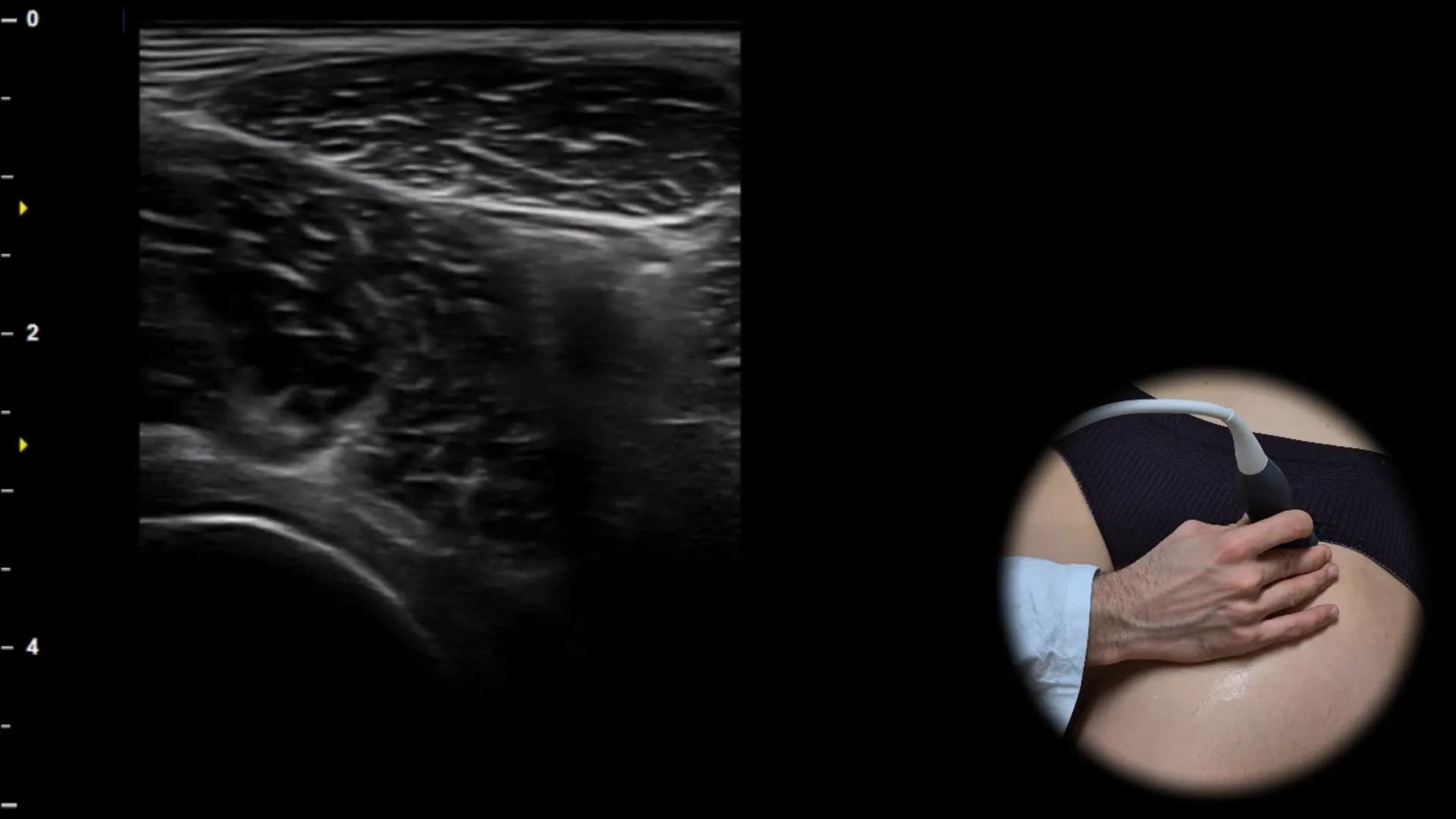
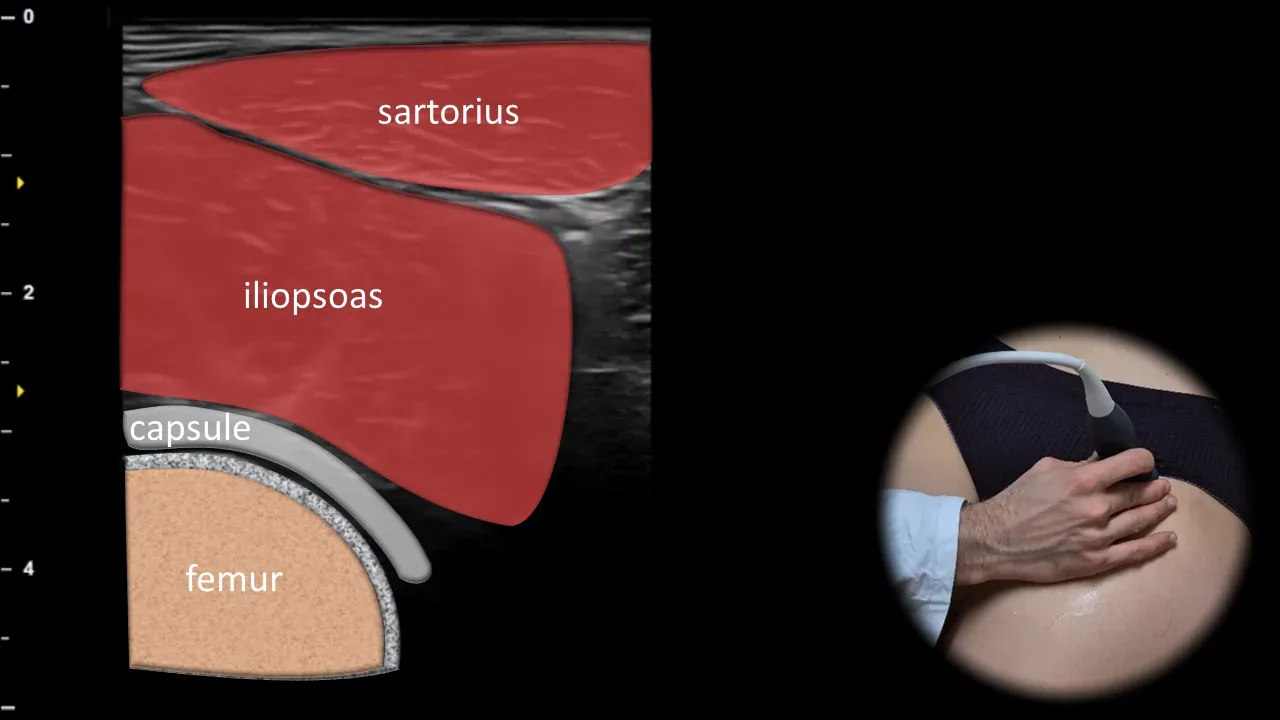
Figure 2. Ventral view, transverse plane.
Transverse ultrasound section of the anterior part of the hip joint. Superficially, the m. sartorius is visible, with the deeper m. iliopsoas below it, under which the joint capsule is shown adjacent to the anterior contour of the femur, which forms the main bony landmark of this projection. This projection is essential for evaluating the anterior recess of the hip joint, particularly for detecting joint effusion, synovitis, and pathology in the area of the m. iliopsoas.

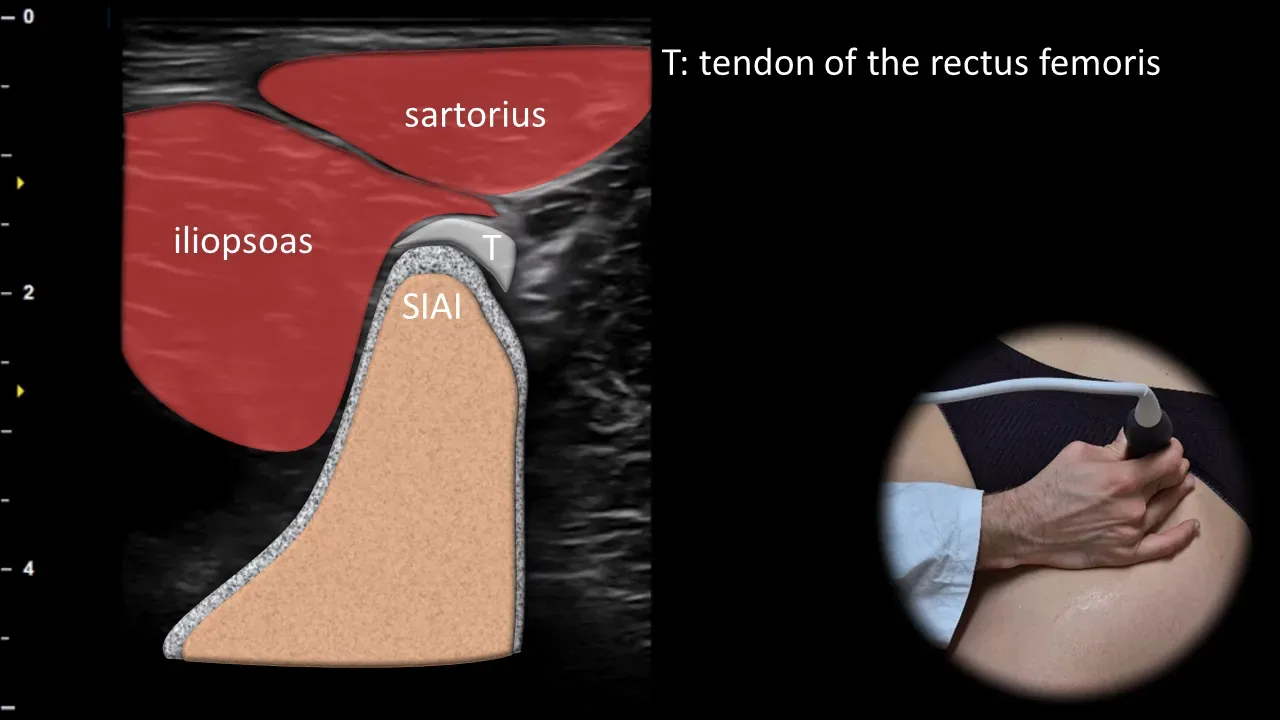
Figure 3. Ventral view, transverse plane. T: rectus femoris muscle tendon, SIAI: spina iliaca anterior inferior
Transverse ultrasound section of the anterior hip region showing the direct tendon of the rectus femoris muscle (T) at its attachment site on the spina iliaca anterior inferior (SIAI). The SIAI is visible as a bony prominence with the adjacent hyperechoic fibrillar tendon, while the sartorius and iliopsoas muscles may also be simultaneously visualized in the surrounding area as important soft tissue landmarks. This projection is essential for evaluating the rectus femoris muscle attachment and for detecting apophyseal injuries, avulsion fractures, and tendinopathy in this region, particularly in athletically active individuals.
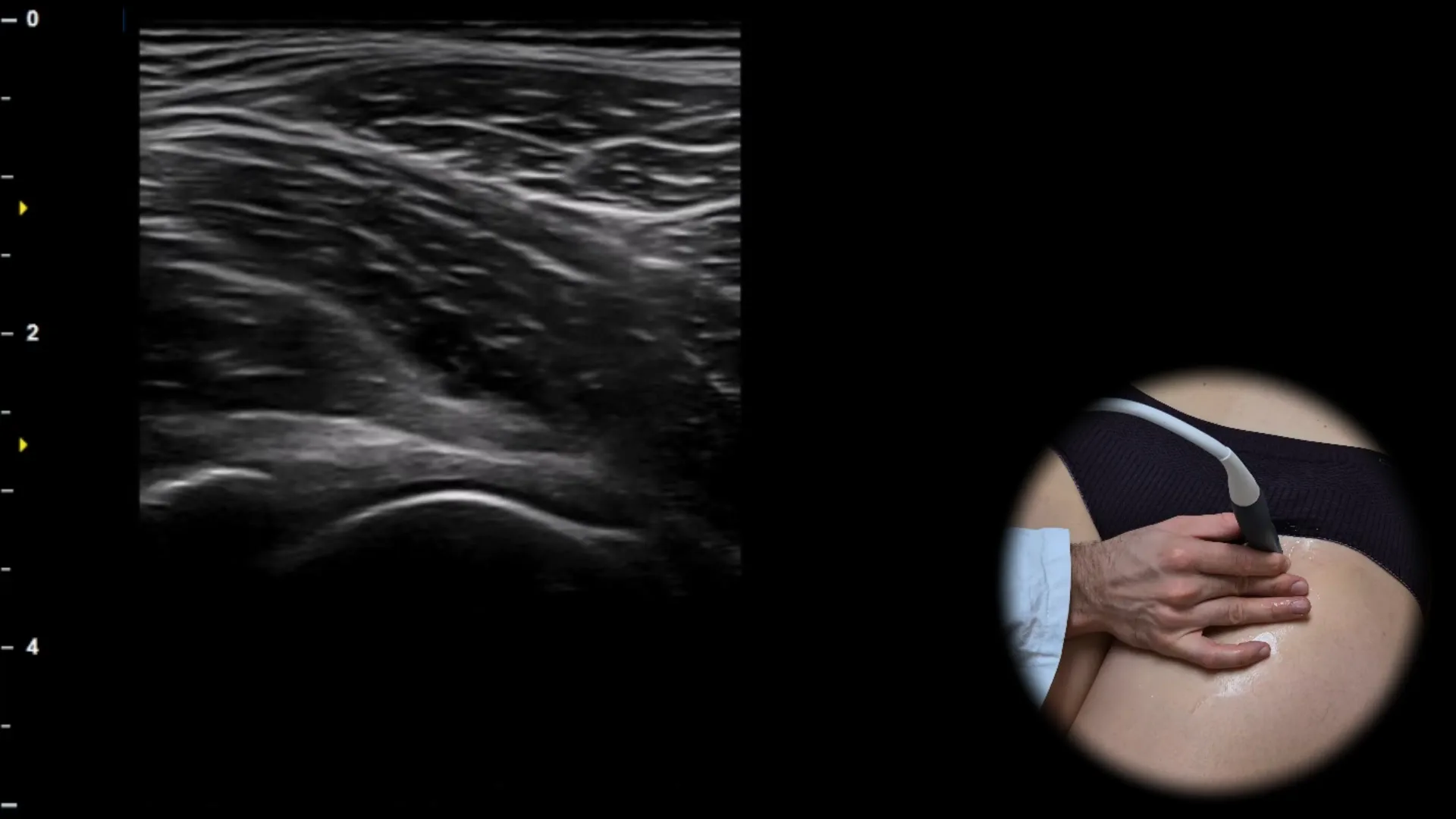
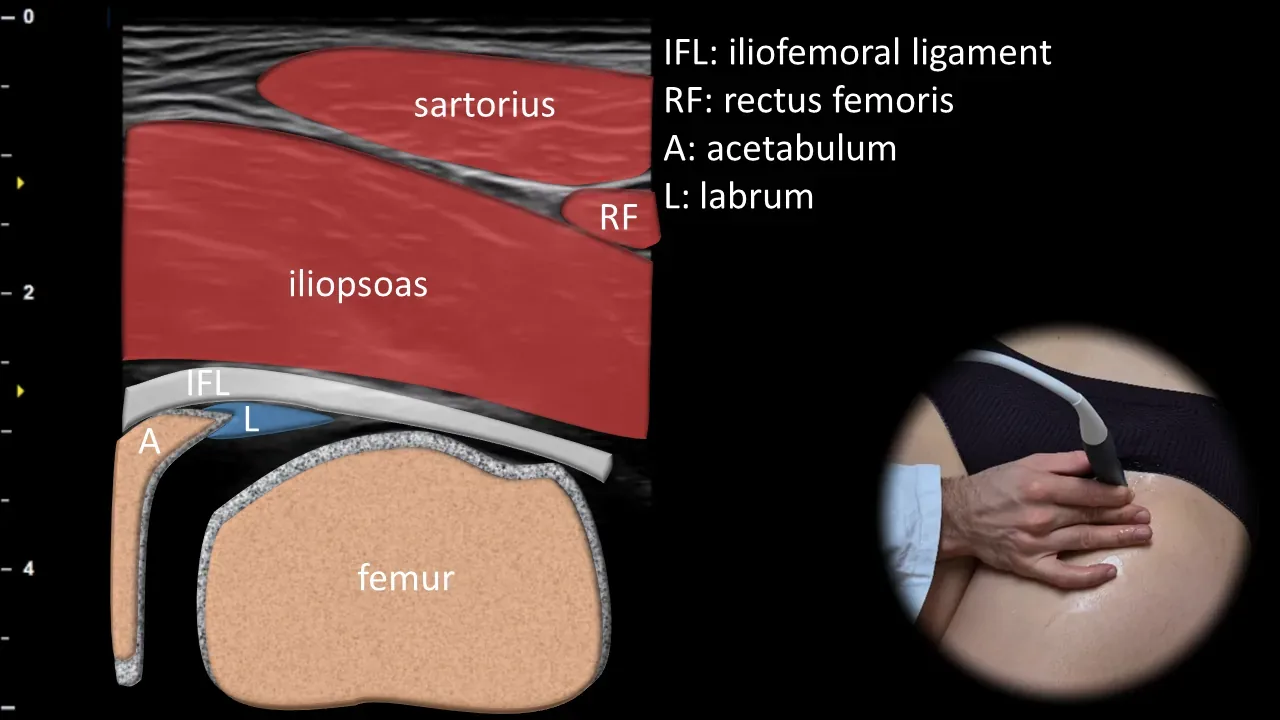
Figure 4. Ventral view, oblique plane. IFL: iliofemoral ligament, A: acetabulum, L: labrum, RF: rectus femoris muscle
Oblique ultrasound section through the anterior part of the hip joint showing the femoroacetabular articulation. The femoral head is visible in articulation with the acetabulum (A), on whose anterior rim the acetabular labrum (L) can be visualized as a triangular structure overlying the bony contour; superficially, the iliofemoral ligament (IFL) is also visible, along with surrounding soft tissue landmarks, particularly the rectus femoris muscle (RF), sartorius muscle, and iliopsoas muscle. This projection is essential for assessing labral integrity, anterior joint congruence, and signs of femoroacetabular impingement.
Clinical Note
In this projection, fluid in the anterior part of the hip joint can be well detected, especially when there is distension of the anterior joint recess.
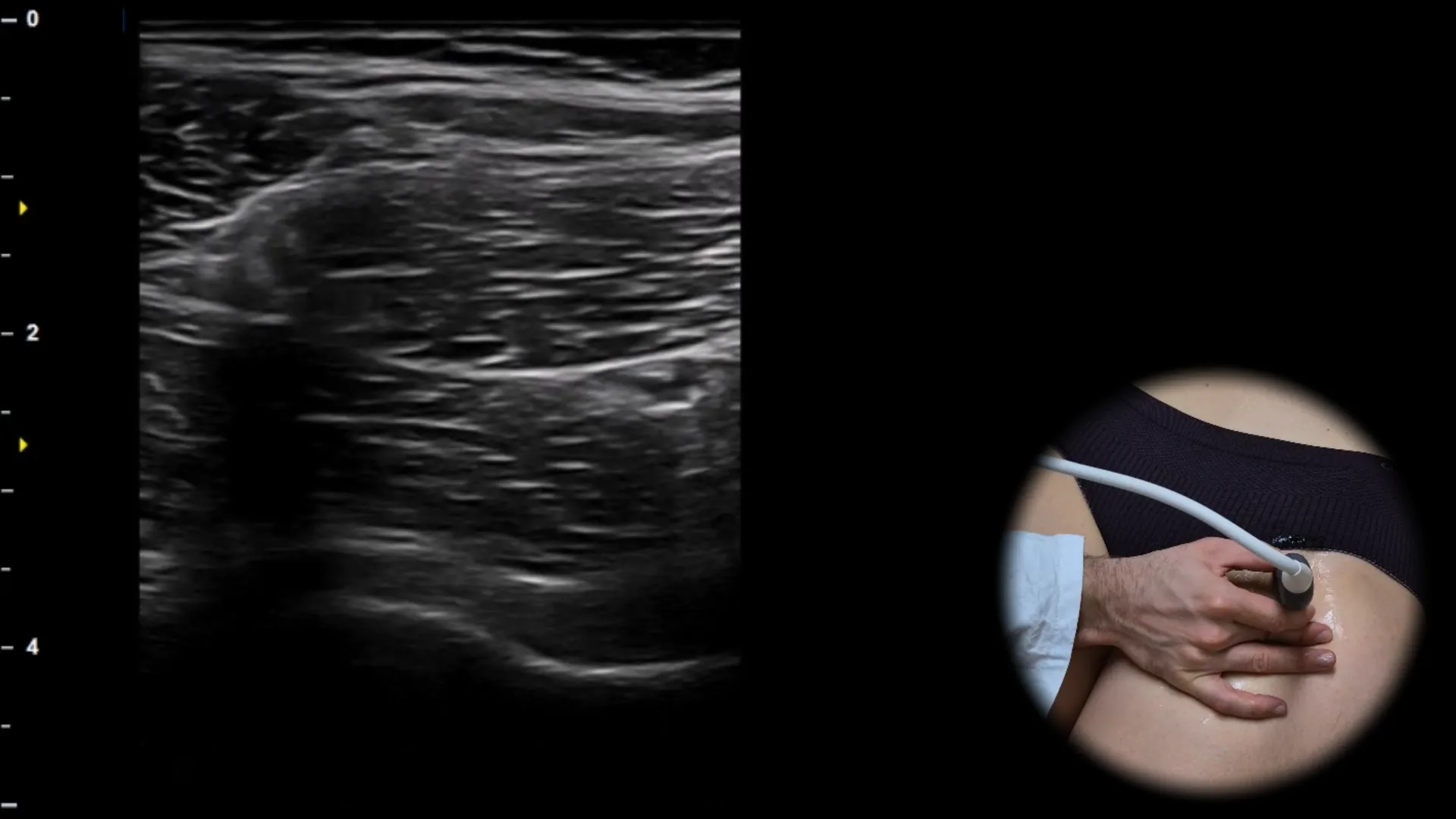
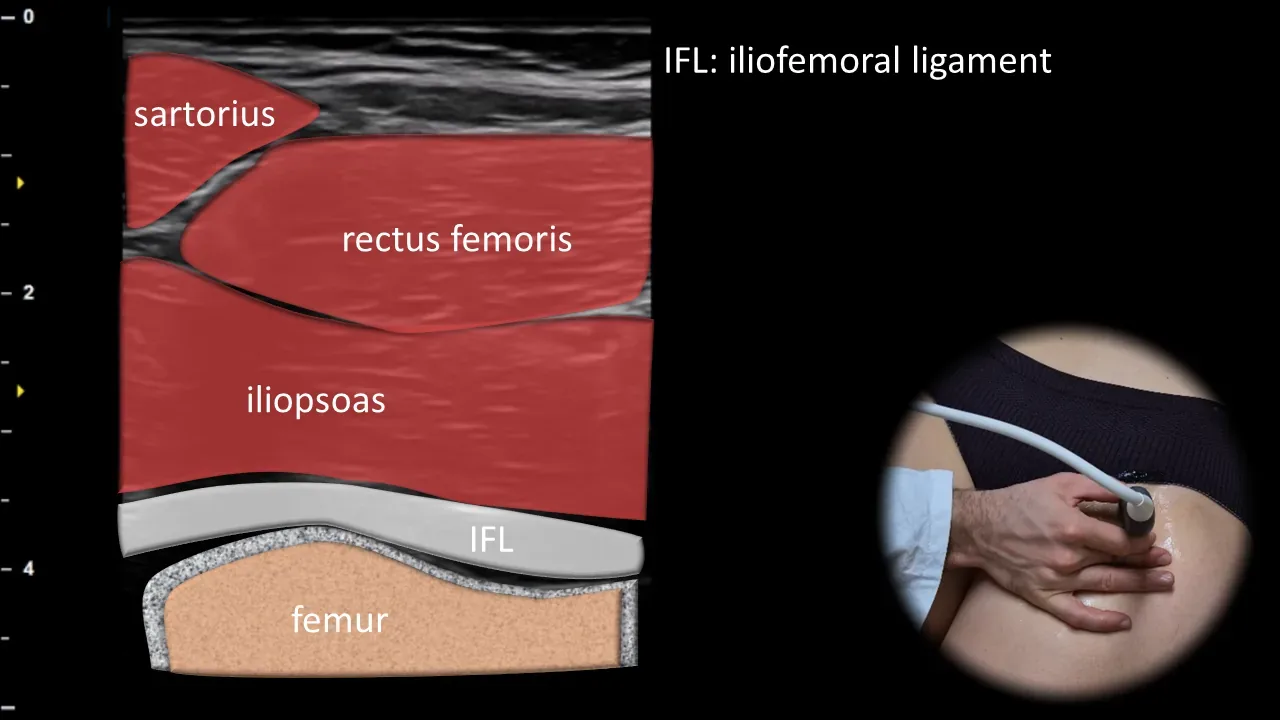
Figure 5. Ventral view, oblique plane. IFL: iliofemoral ligament
Oblique ultrasound section through the anterior part of the hip joint taken more distally, showing the anterior joint recess in the region of the femoral head. Beneath the superficially located muscles, particularly the rectus femoris, sartorius, and iliopsoas muscles, the joint capsule is visible, and beneath it runs the iliofemoral ligament (IFL), which appears as a hyperechoic band adjacent to the anterior contour of the femur. This projection is crucial for evaluating joint effusion, synovitis, and thickening of the anterior capsule or iliofemoral ligament in inflammatory and degenerative diseases of the hip joint.
Clinical Note
When an intra-articular collection is present, anterior recess bulging may occur and the iliofemoral ligament may be displaced ventrally, which increases the conspicuity of the effusion in this projection.
2. Medial View
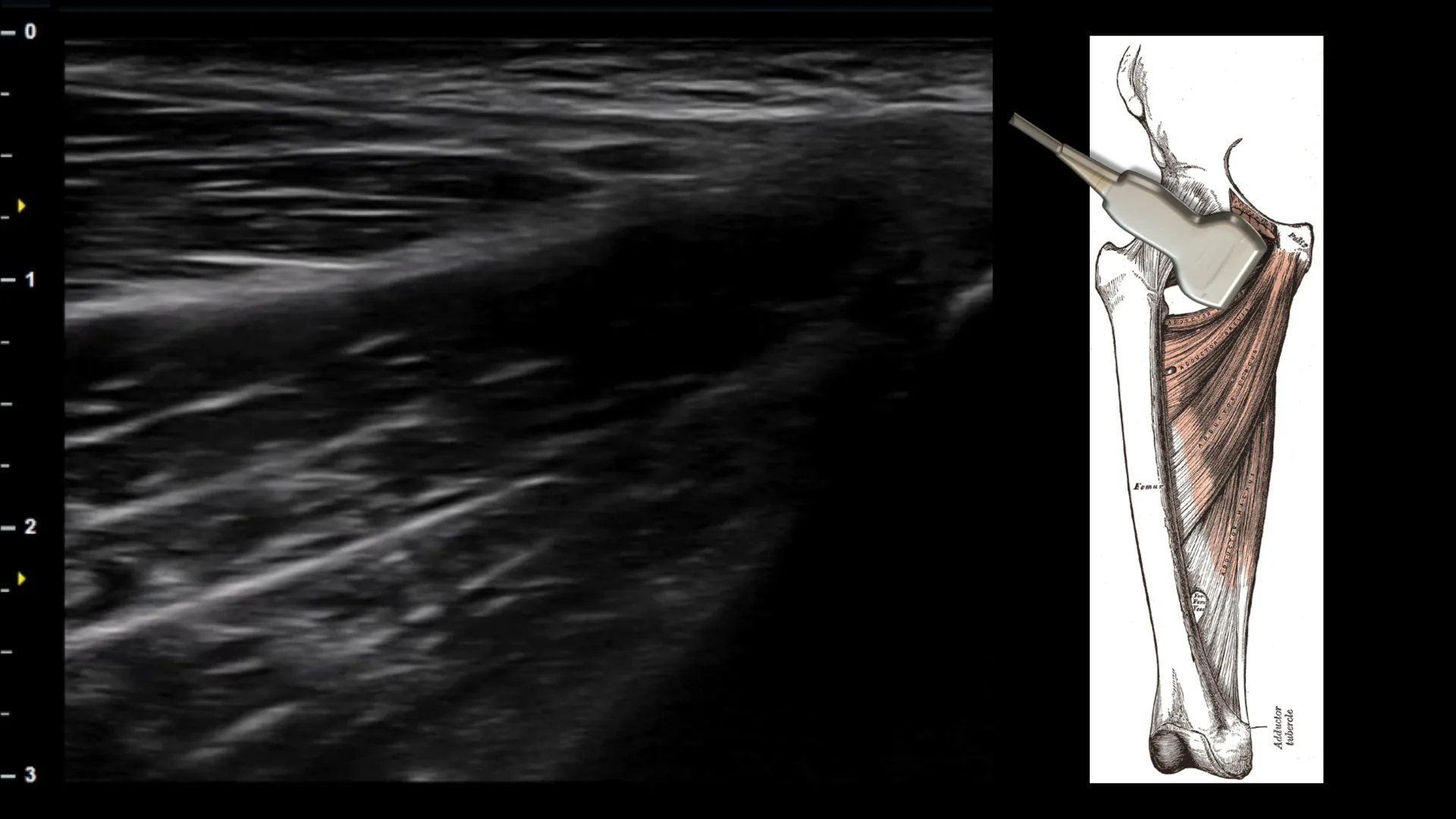
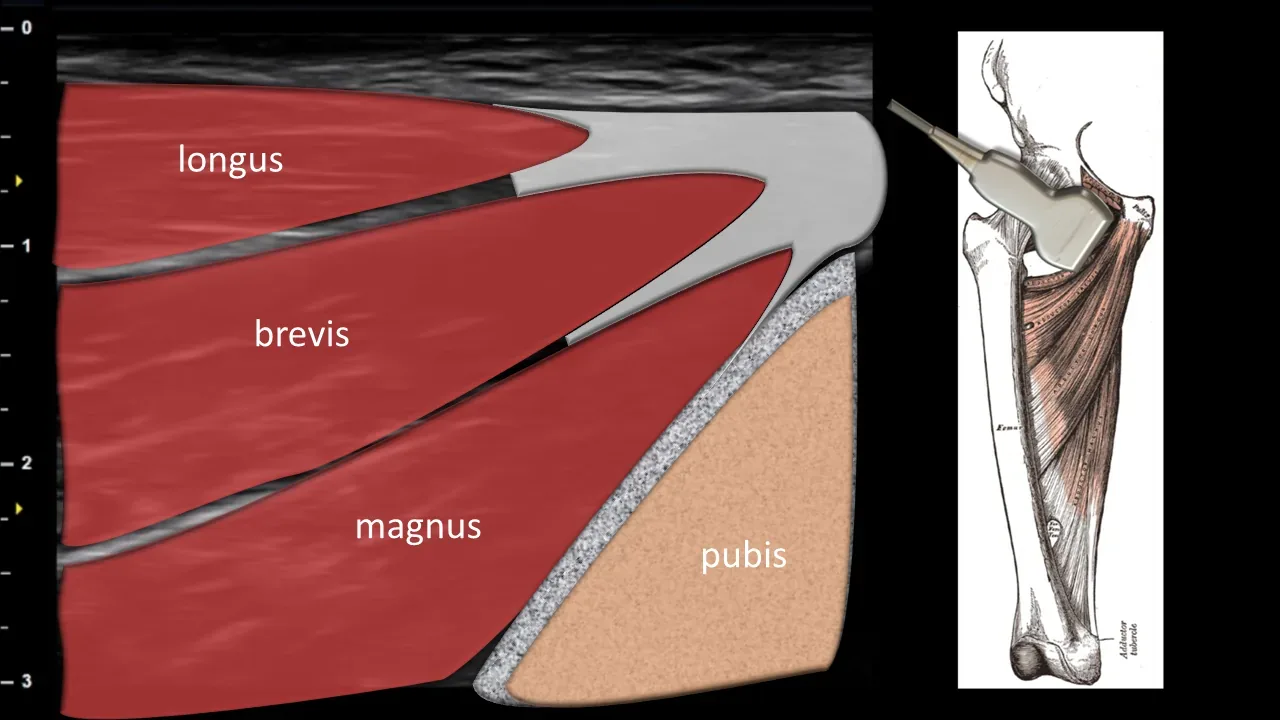
Figure 6. Medial view, transverse plane. adductors
Transverse ultrasound section of the medial thigh displaying the adductor muscle group. In this projection, the muscles are arranged in layers above each other, superficially the adductor longus, beneath it the adductor brevis, and deepest the adductor magnus, which allows clear visualization of their mutual anatomical relationships. This projection is important for assessment of the adductor musculature and for detection of muscle ruptures, hematomas, or other pathological changes in the medial thigh region.
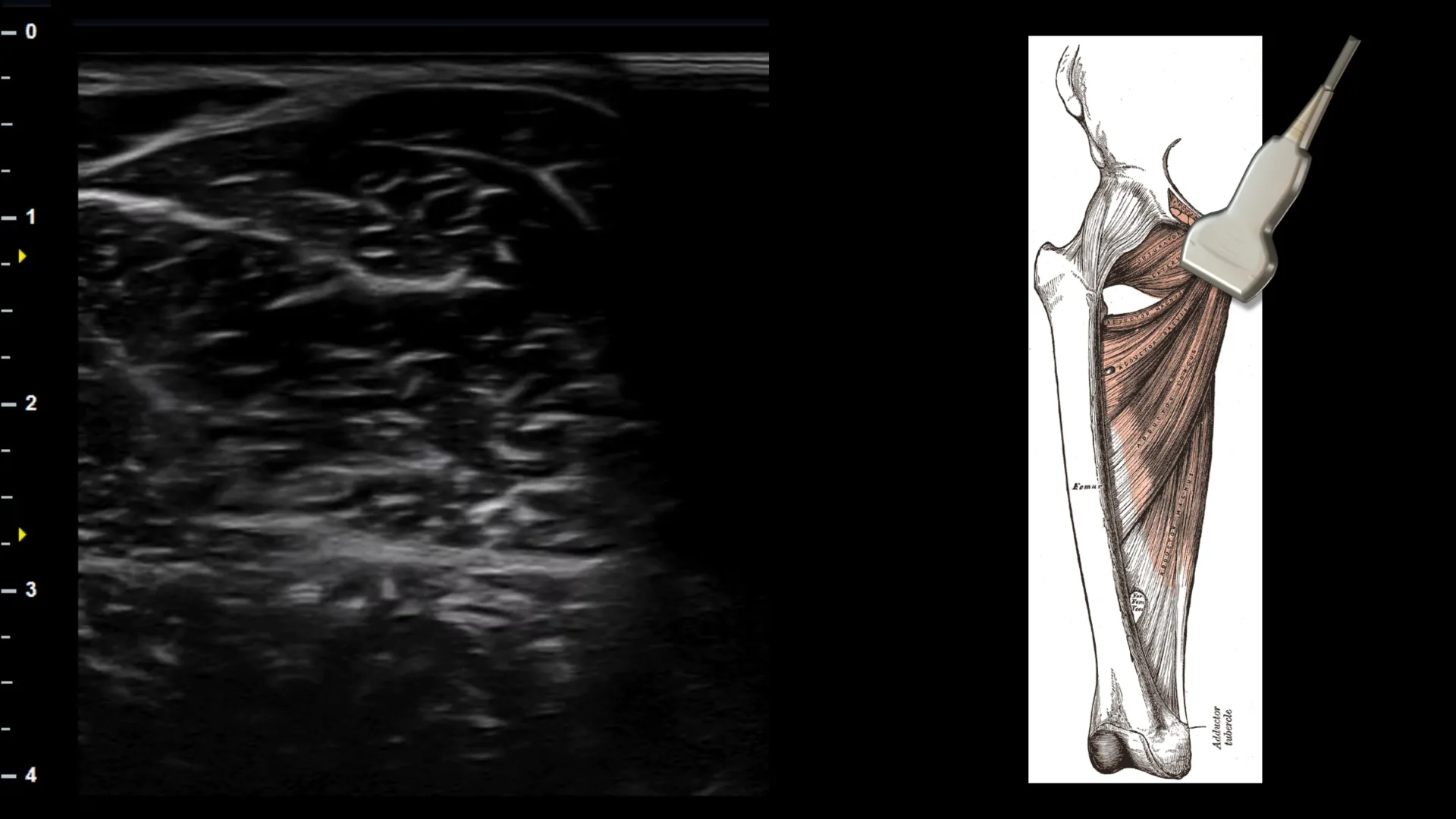
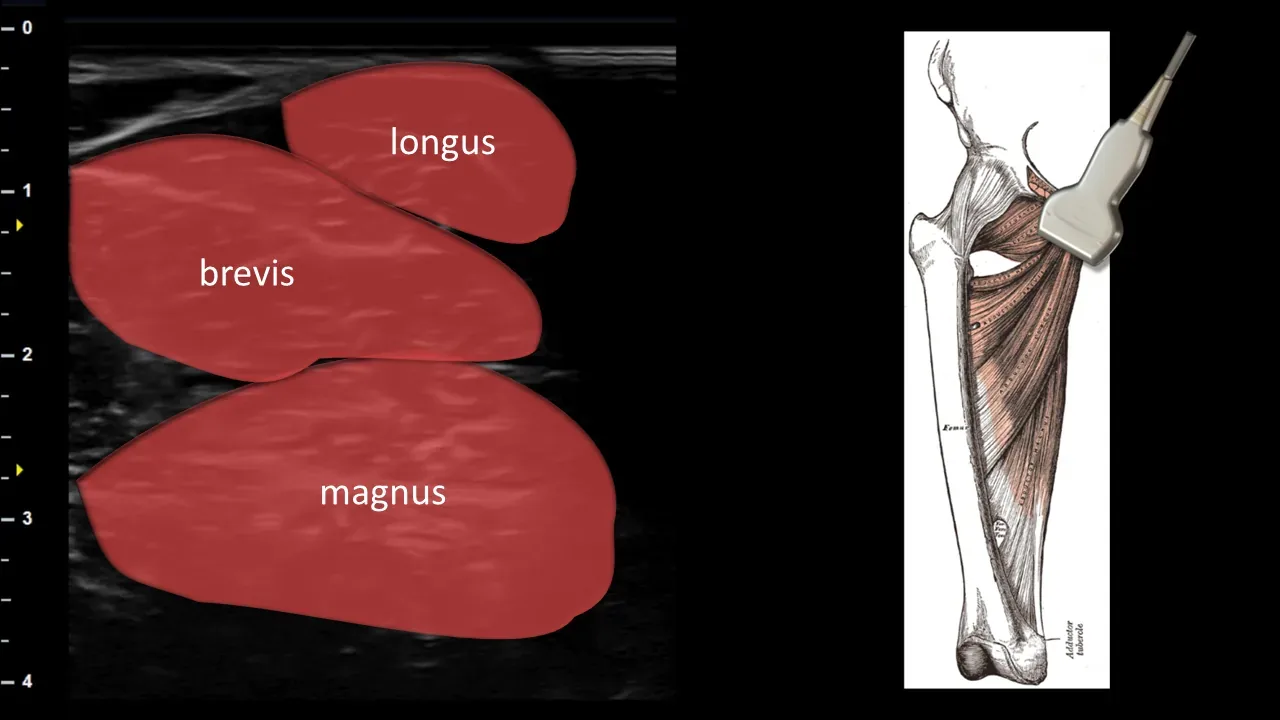
Figure 7. Medial view, oblique plane. adductor attachment to the pubic bone
Oblique ultrasound section of the medial part of the groin focused on the area of adductor muscle attachment to the os pubis. In this projection, individual layers of the adductors are visible, particularly m. adductor longus, m. adductor brevis and m. adductor magnus, extending toward their proximal attachment to the pubic bone, which allows clear visualization of their mutual anatomical relationships in the enthesis area. This projection is crucial for assessing the continuity of the adductor attachment tendon and for detecting enthesopathy, partial ruptures or other pathological changes in the pubic bone area.
3. Lateral View
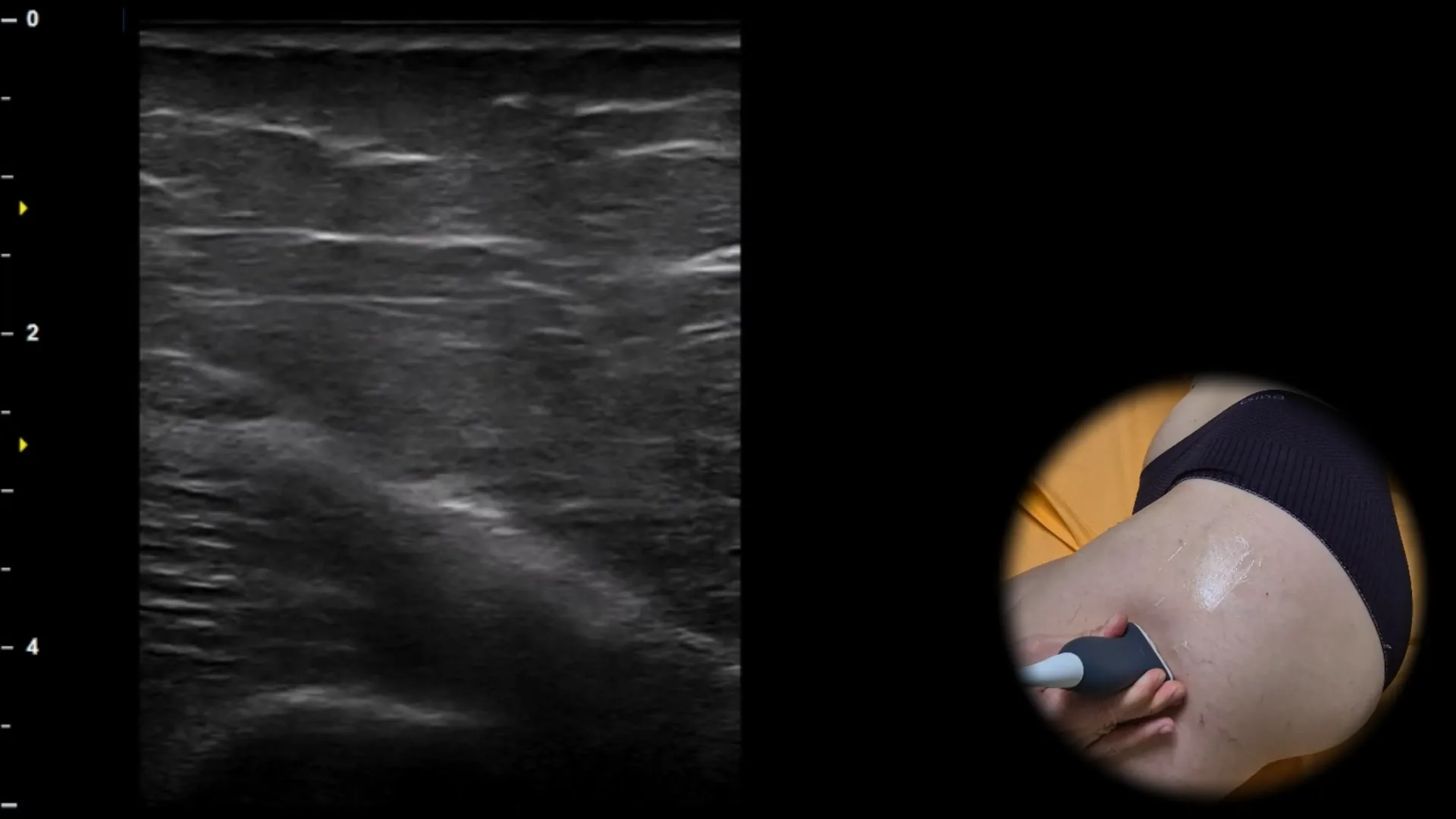

Figure 8. Lateral view, transverse plane.
Transverse ultrasound section of the lateral portion of the thigh at the distal level, where the m. vastus lateralis is visible superficially as a hypoechoic muscle layer with fine internal fibrous bands. Deeper, the cortical contour of the femur is displayed as a continuous curved hyperechoic line with dorsal acoustic shadowing, which represents the main bony landmark of this projection. This view serves primarily to identify the femur and as a reference starting level for its proximal tracking toward the greater trochanter.
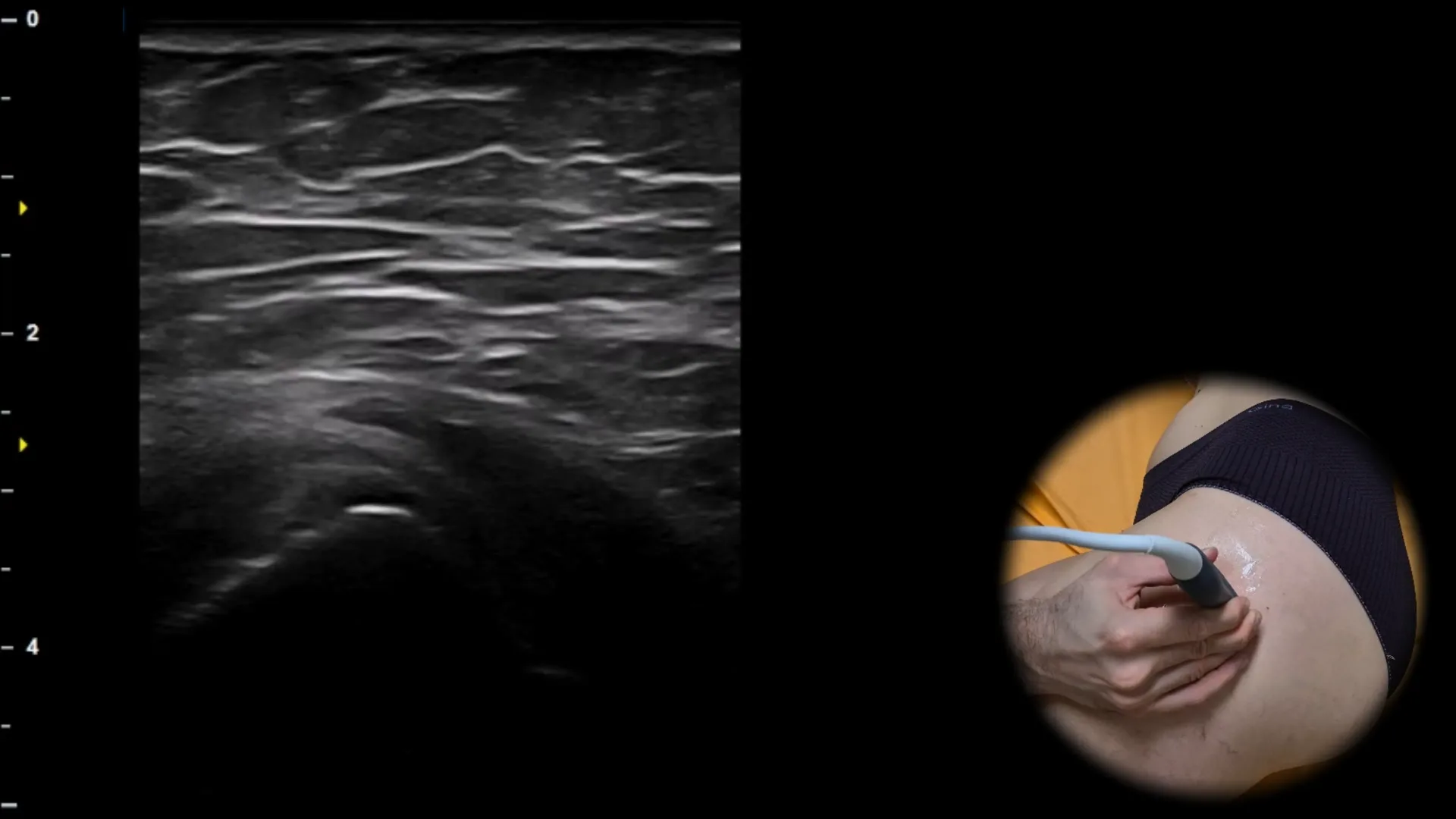
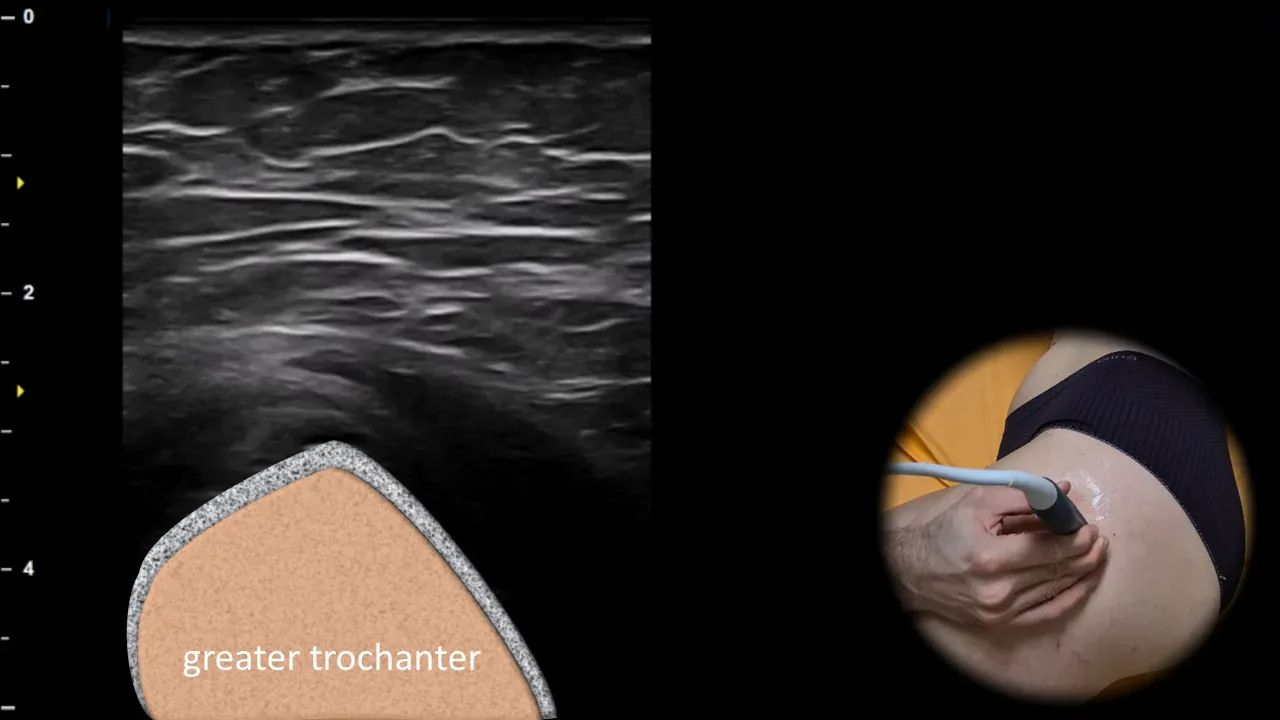
Figure 9. Lateral view, transverse plane.
Transverse ultrasound section of the lateral part of the hip region with proximal displacement of the probe along the femur. At this level, the originally round shape of the femur changes to a more pronounced triangular to pyramidal bone contour, which corresponds to the greater trochanter area and represents an important landmark during sonographic examination of the lateral hip. Correct identification of the greater trochanter is essential for subsequent evaluation of surrounding tendon attachments and bursae in this region.
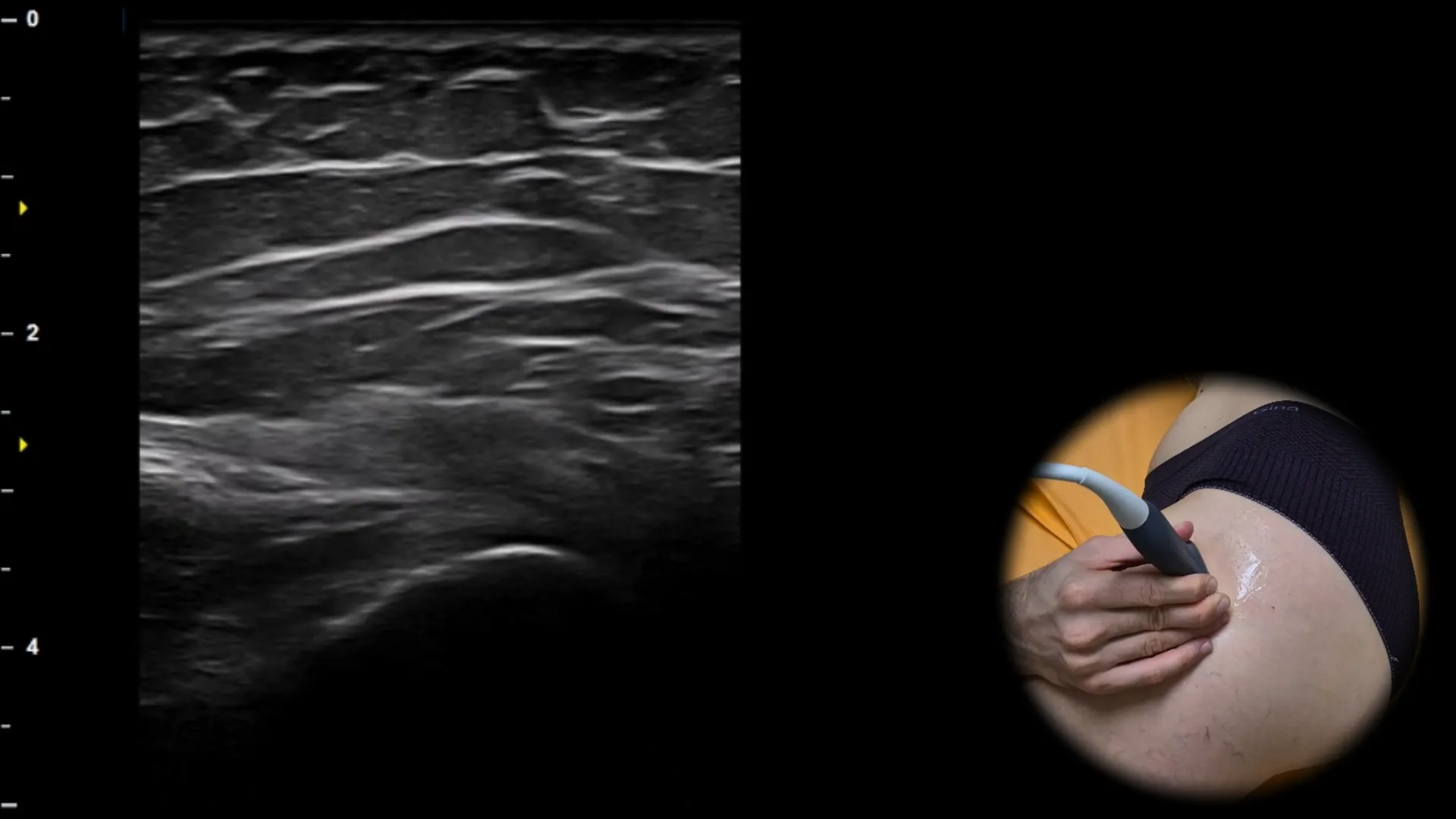
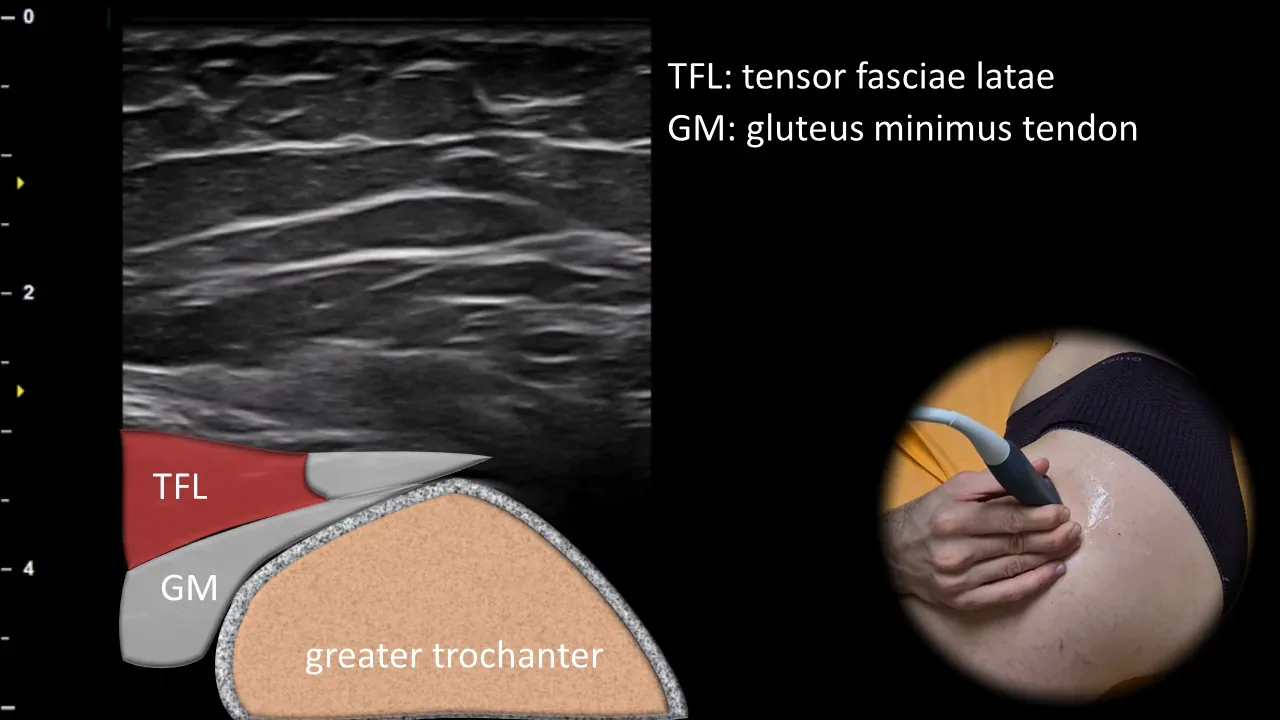
Figure 10. Lateral view, oblique plane. TFL: m. tensor fasciae latae, GM: m. gluteus minimus tendon
Oblique ultrasound section of the lateral part of the hip region focused on the anterior facet of the greater trochanter. Superficially and laterally, the m. tensor fasciae latae (TFL) is visible, beneath which runs the m. gluteus minimus tendon (GM) inserting on the anterior facet of the greater trochanter and appearing as a well-defined fibrillar hyperechoic band. This projection is essential for evaluating the insertion of the m. gluteus minimus tendon and for detecting tendinopathy or partial ruptures of gluteal tendons in patients with lateral hip pain.
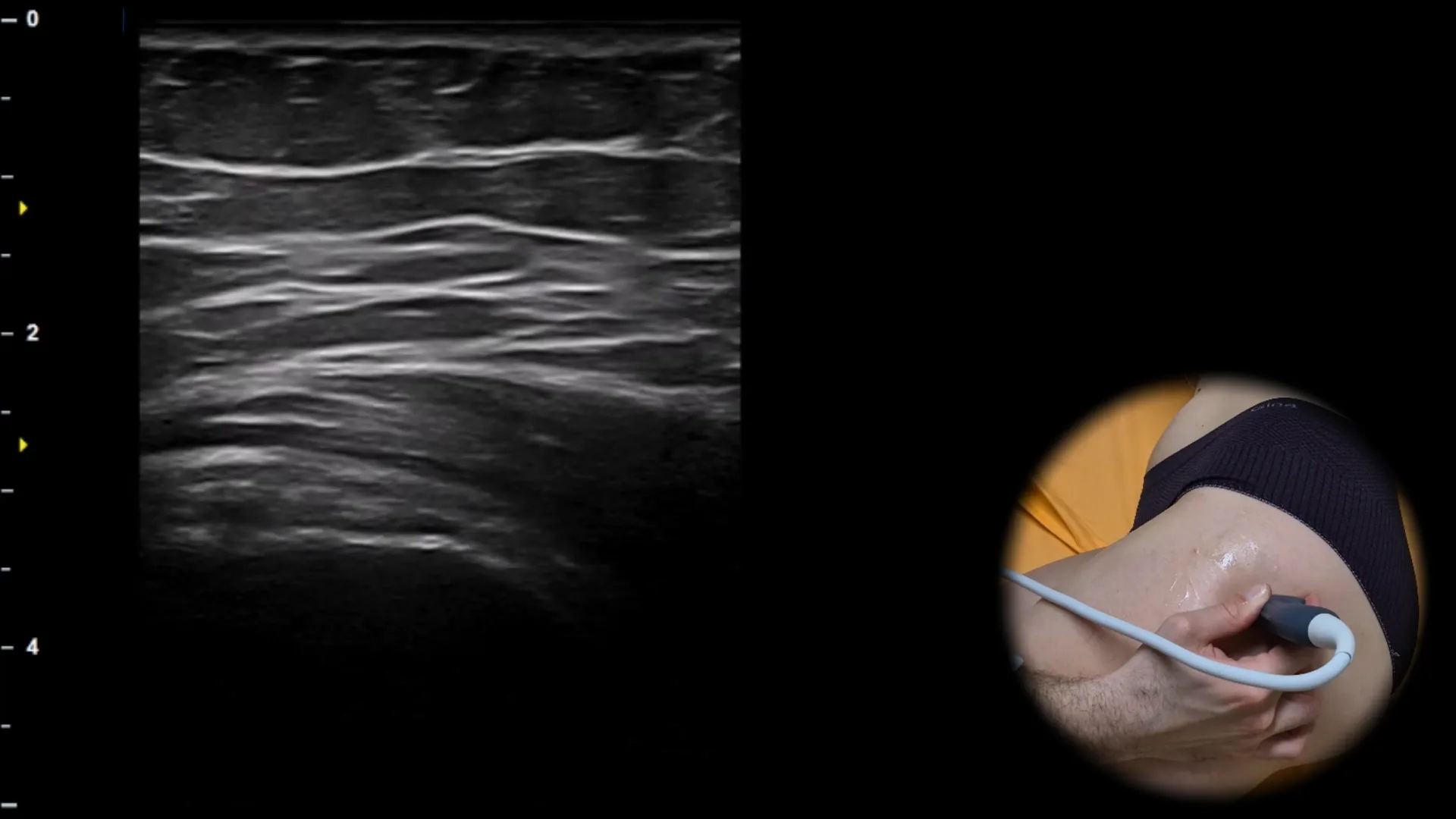
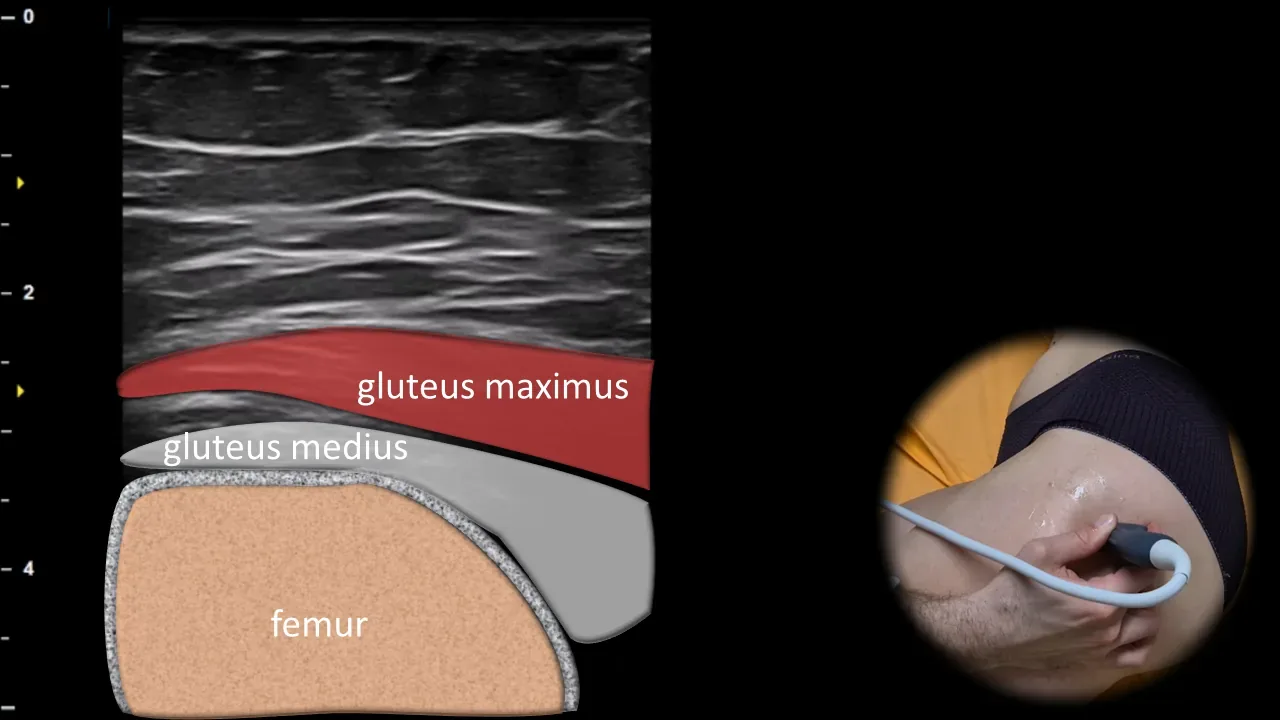
Figure 11. Lateral view, oblique plane.
Oblique ultrasound section of the lateral part of the hip region showing the greater trochanter area. Superficially, the m. gluteus maximus is visible, beneath it the tendon of m. gluteus medius adjacent to the lateral facet of the greater trochanter, with the bone contour of the proximal femur depicted deeply as the main landmark of this projection. This projection is essential for evaluating the insertion of m. gluteus medius and for detecting tendinopathy, partial ruptures, and changes in the peritrochanteric bursae in patients with lateral hip pain.
4. Dorsal View
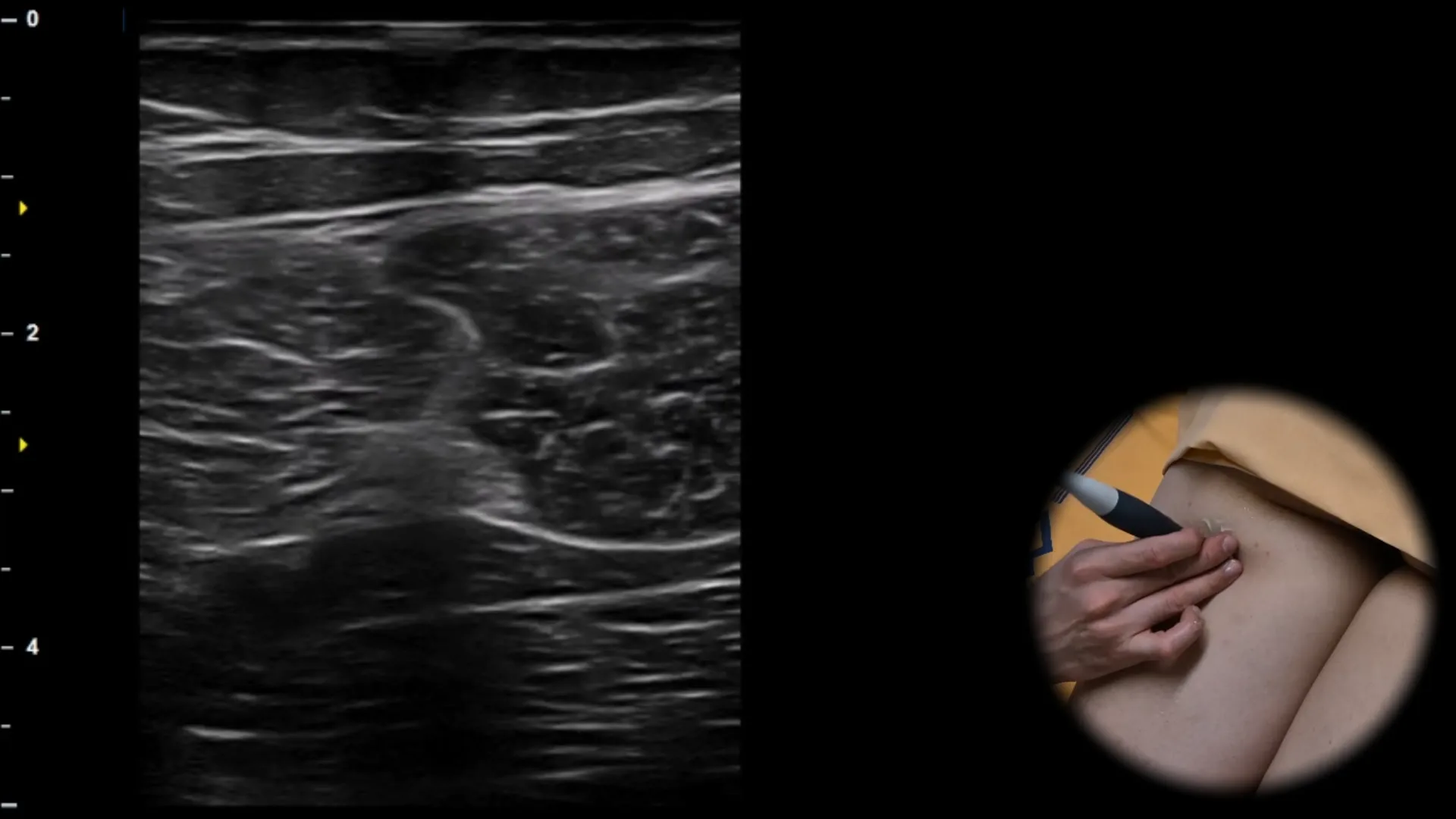
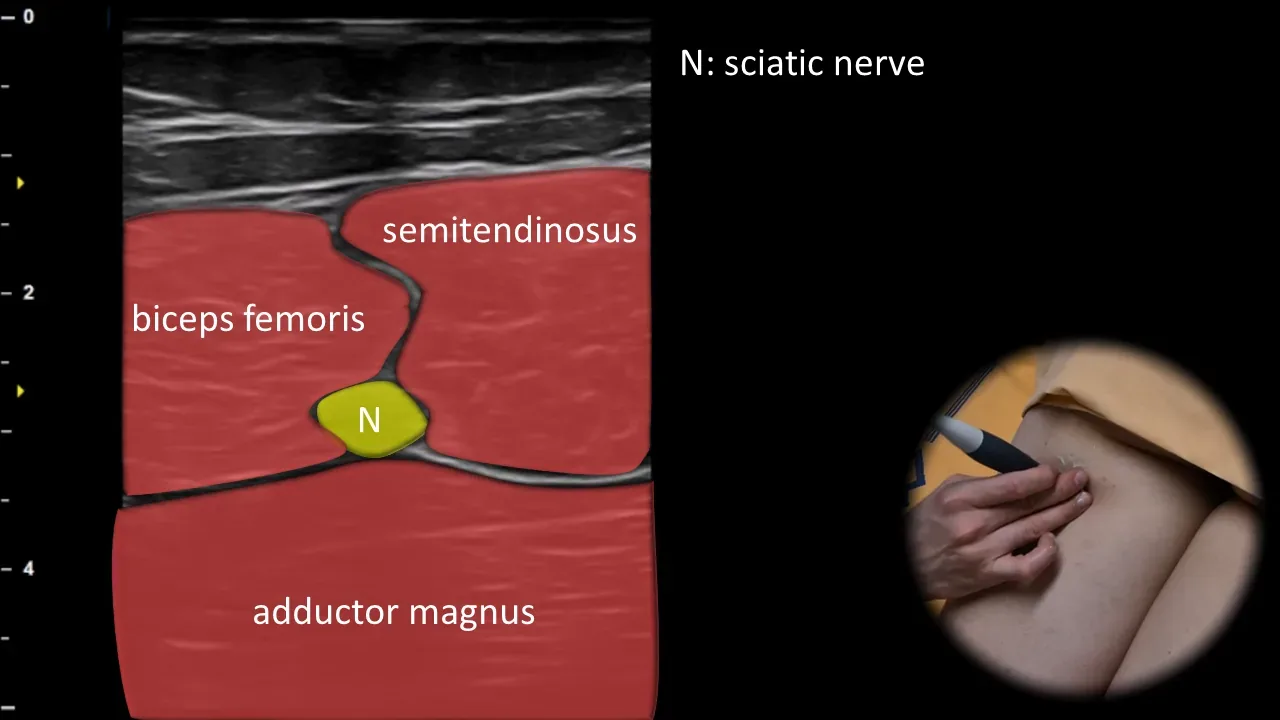
Figure 12. Dorsal view, transverse plane. N: n. ischiadicus
Transverse ultrasound section of the posterior thigh showing the n. ischiadicus as an oval structure with typical fascicular appearance, located between the m. semitendinosus medially and the long head of the m. biceps femoris laterally. Deeper, the m. adductor magnus is visible, forming the floor of this anatomical window. This projection is essential for localization of the n. ischiadicus and for assessment of its pathology in the posterior thigh region. Clinical note: the typical arrangement of surrounding muscles creates the so-called "windmill sign," which facilitates rapid orientation and identification of the nerve during sonographic examination.
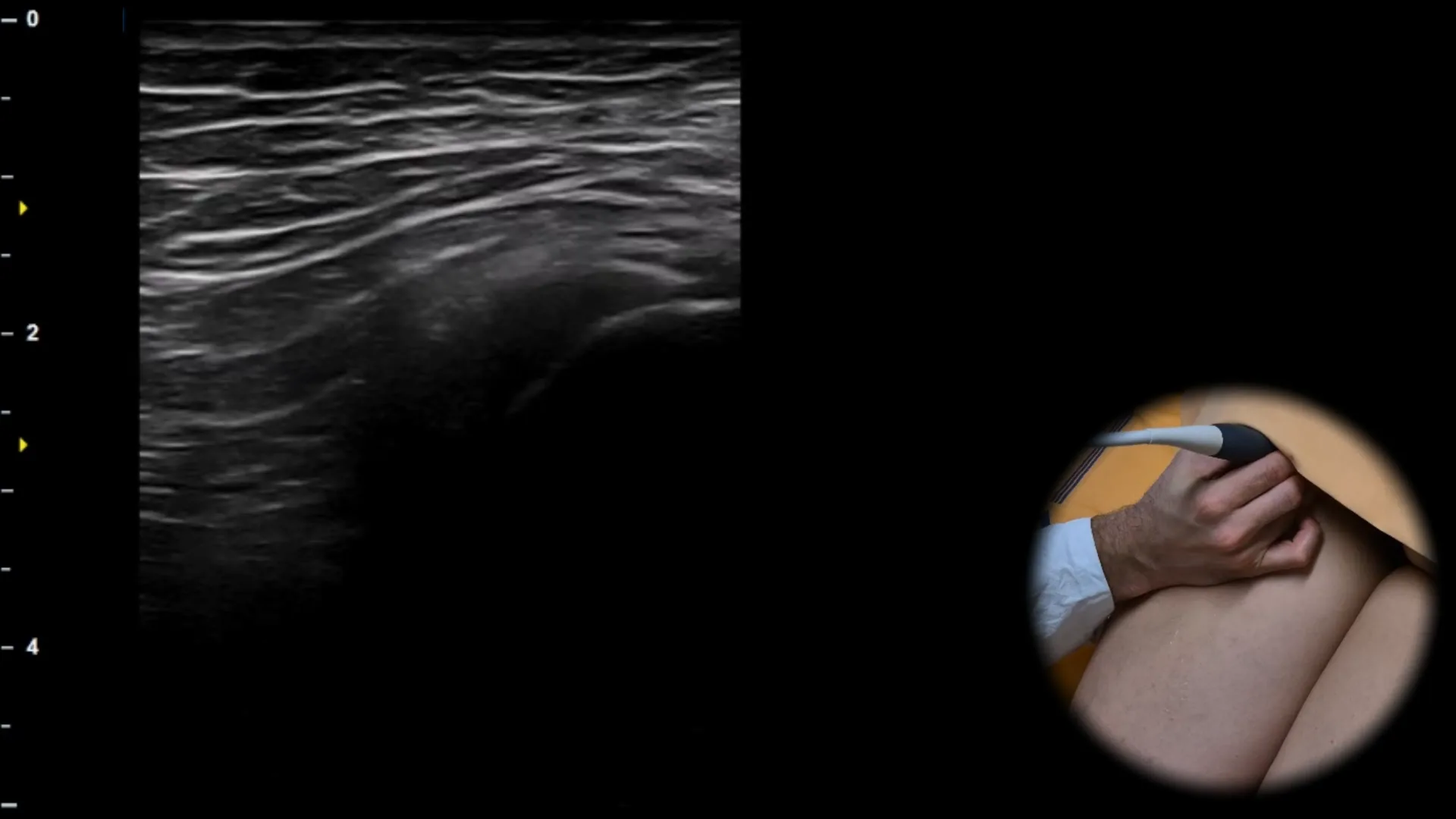
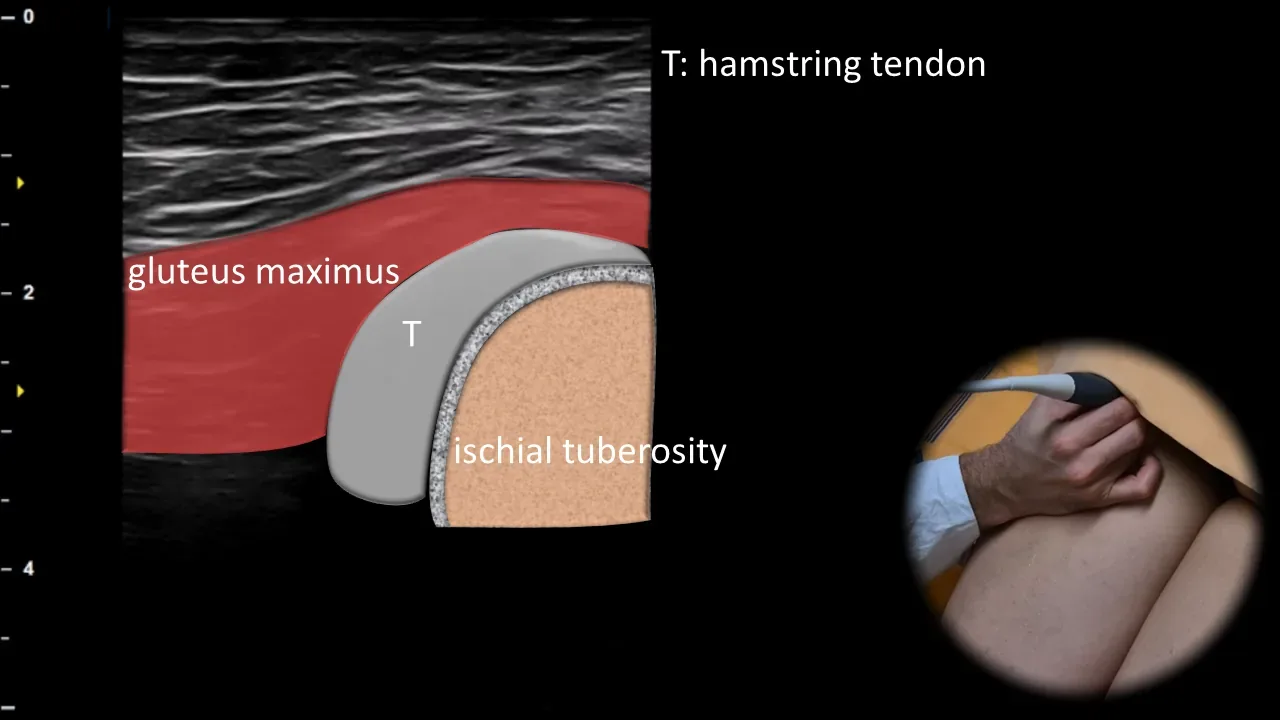
Figure 13. Dorsal view, transverse plane. T: hamstring tendon
Transverse ultrasound section of the proximal posterior thigh showing the ischial tuberosity region. The ischial tuberosity appears as an arched hyperechoic bony contour, onto which attaches the common tendinous insertion of the hamstrings (T), including the tendons of m. semitendinosus, m. semimembranosus and the long head of m. biceps femoris; superficially, m. gluteus maximus is also visible. This projection is essential for evaluating the proximal hamstring insertion and for detecting tendinopathy, partial ruptures or avulsion injuries in the ischial tuberosity region, especially in the athletic population.
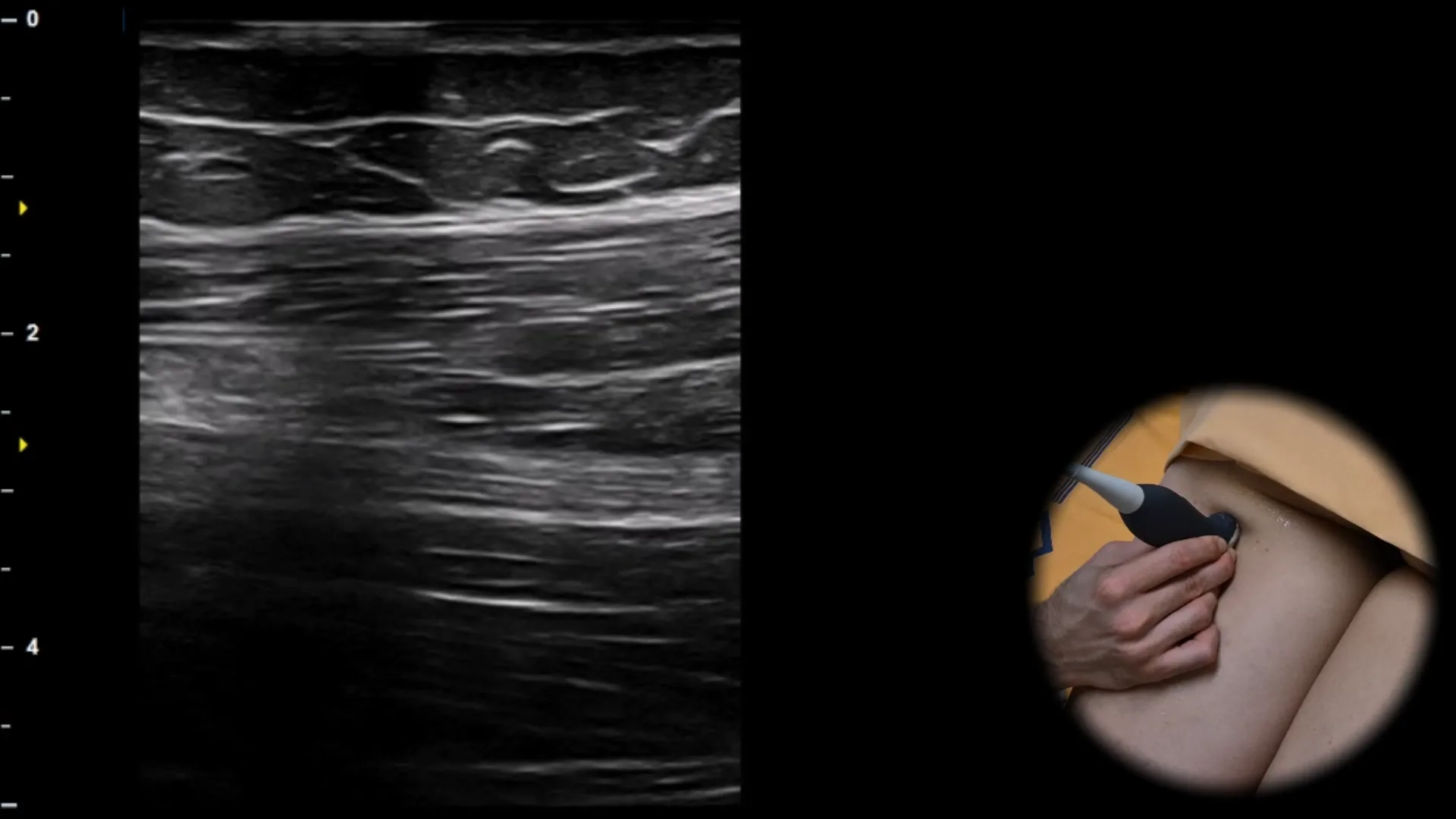
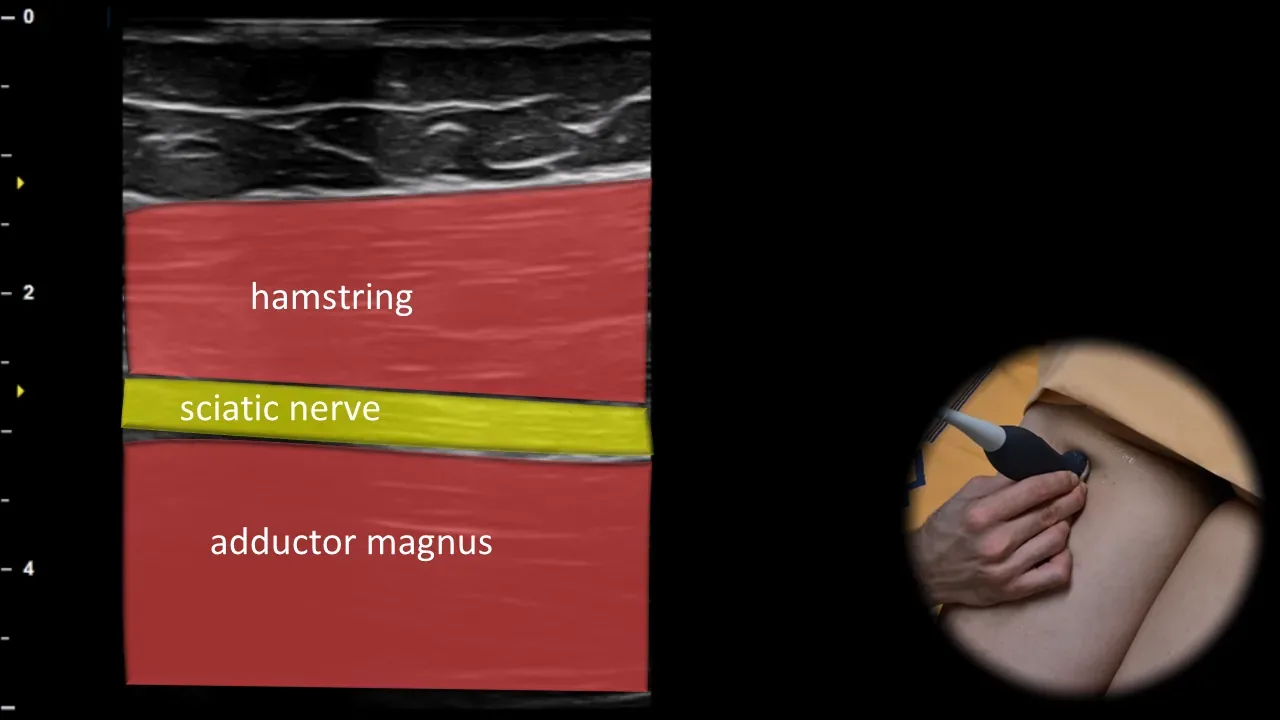
Figure 14. Dorsal view, sagittal plane.
Longitudinal ultrasound section of the posterior thigh showing the n. ischiadicus in long axis. The nerve is visible in this projection as a striated structure with typical fascicular arrangement, running between the hamstrings superficially and m. adductor magnus deeper. This projection is essential for assessing continuity of the n. ischiadicus, its course, and for detection of pathological changes in the posterior thigh region.
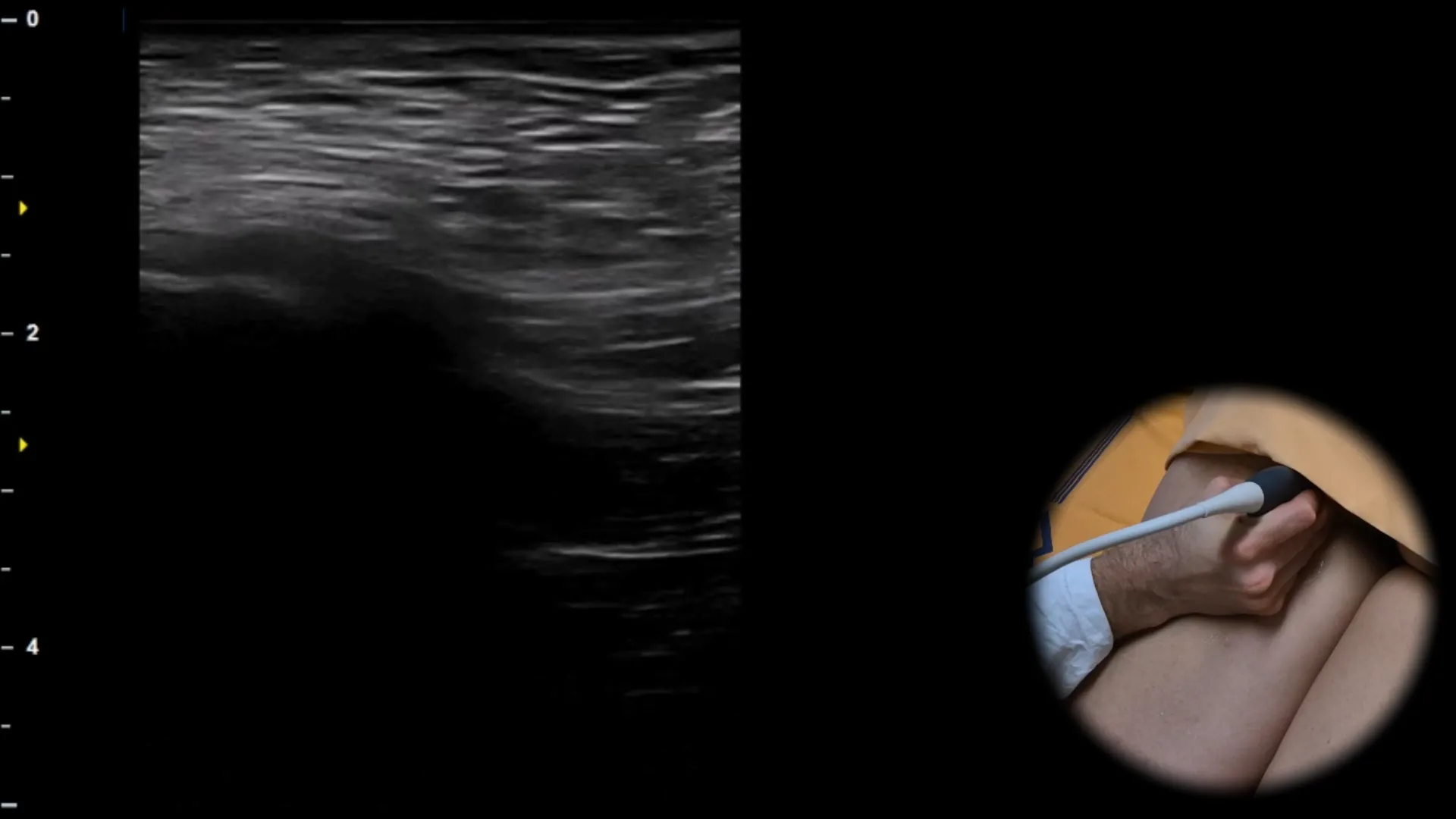
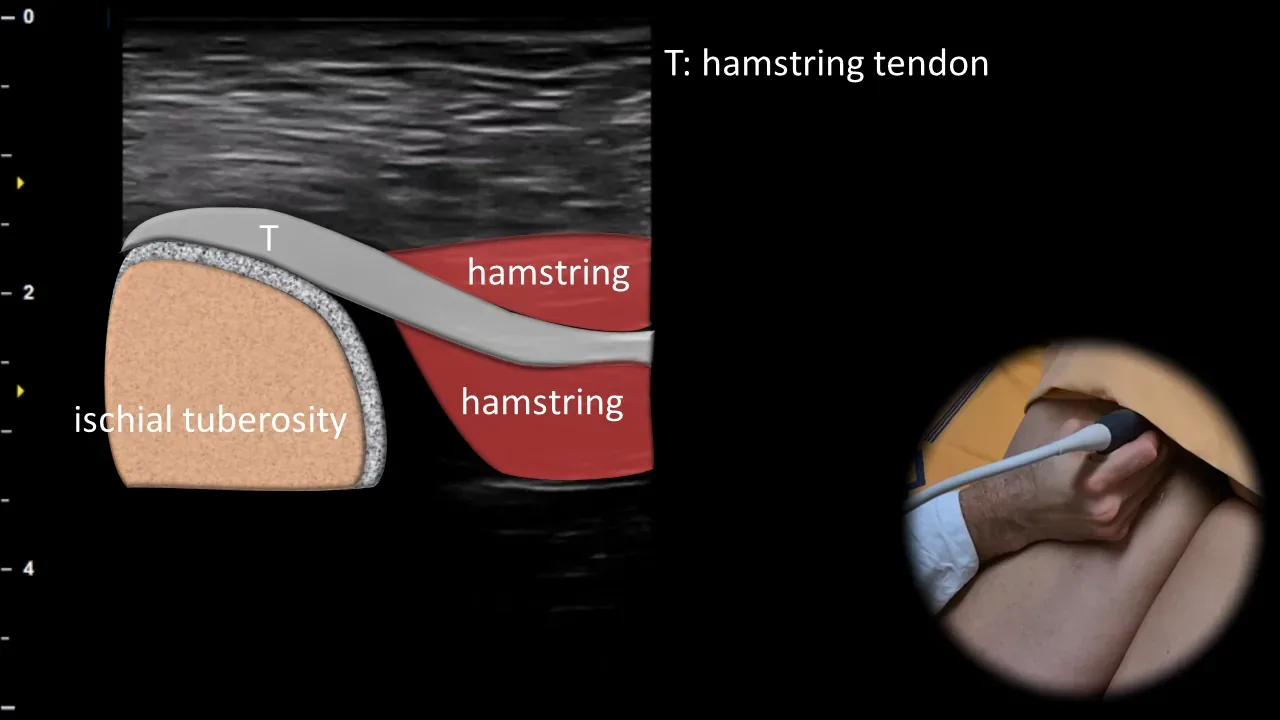
Figure 15. Dorsal view, sagittal plane. T: hamstring tendon
Longitudinal ultrasound section of the tuber ischiadicum area showing the common hamstring insertion. The tuber ischiadicum is visible as a curved hyperechoic bony contour, to which the common tendinous origin of the hamstrings (T) attaches, including the tendons of m. semitendinosus, m. semimembranosus and the long head of m. biceps femoris; distally from the insertion, the tendon transitions into the muscle bellies of the posterior thigh muscle group. This projection is essential for evaluating the proximal hamstring insertion and for detecting tendinopathy, partial ruptures and complete avulsions, particularly in athletes with pain in the gluteal region or posterior thigh.
Unlock the full Health Library
Full access to scanning protocols, anatomy, and clinical references. Cancel anytime.
- Every protocol and anatomy reference
- Original ultrasound illustrations and video demonstrations
- Sync across mobile and web