Ultrasound examination
Examination Protocol
Ventral view
- Transverse plane
- Sagittal plane
Medial view
- Frontal plane
Lateral view
- Frontal plane
Dorsal view
- Transverse plane
Interactive feature, available in the app
1. Ventral view
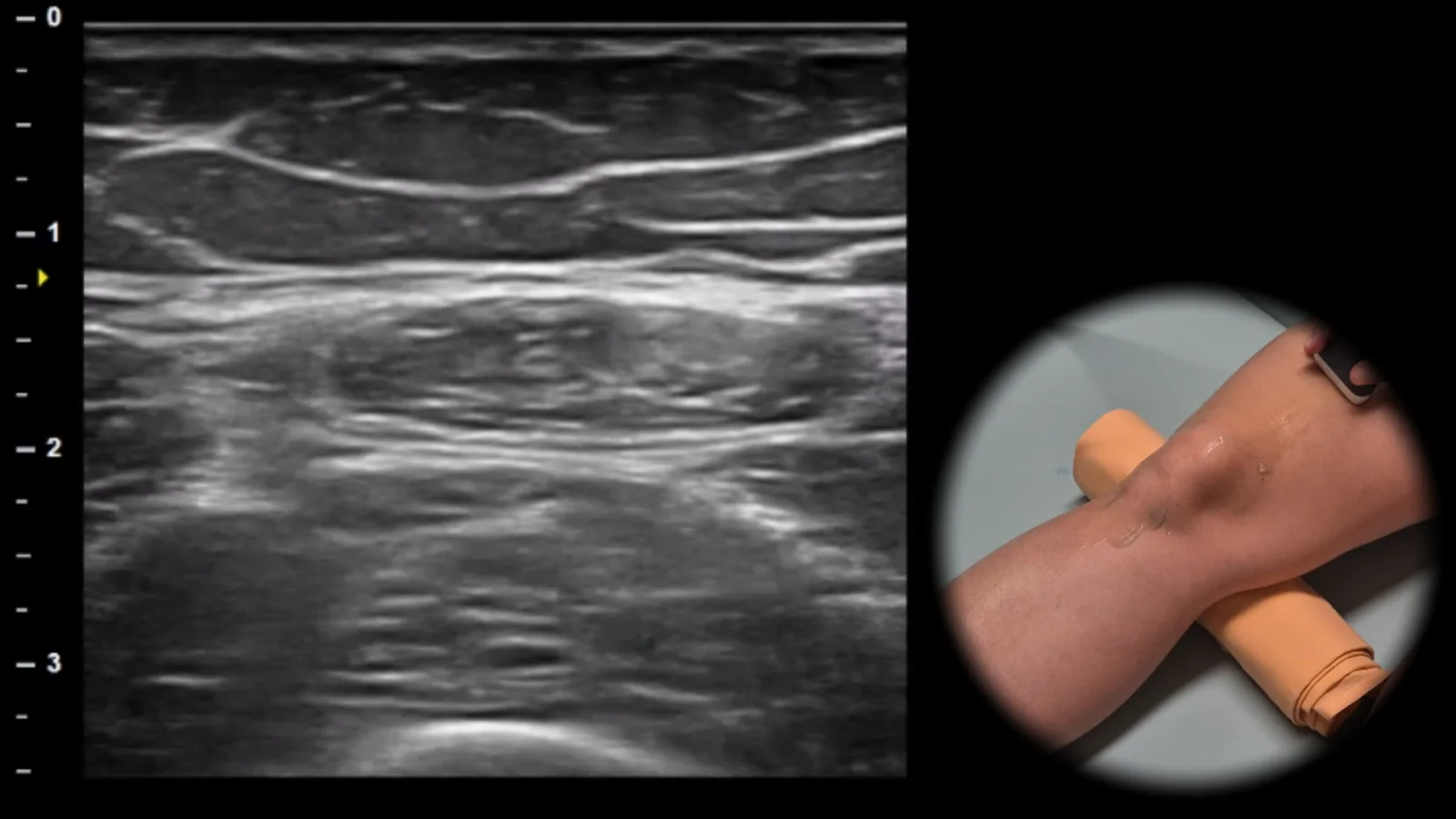
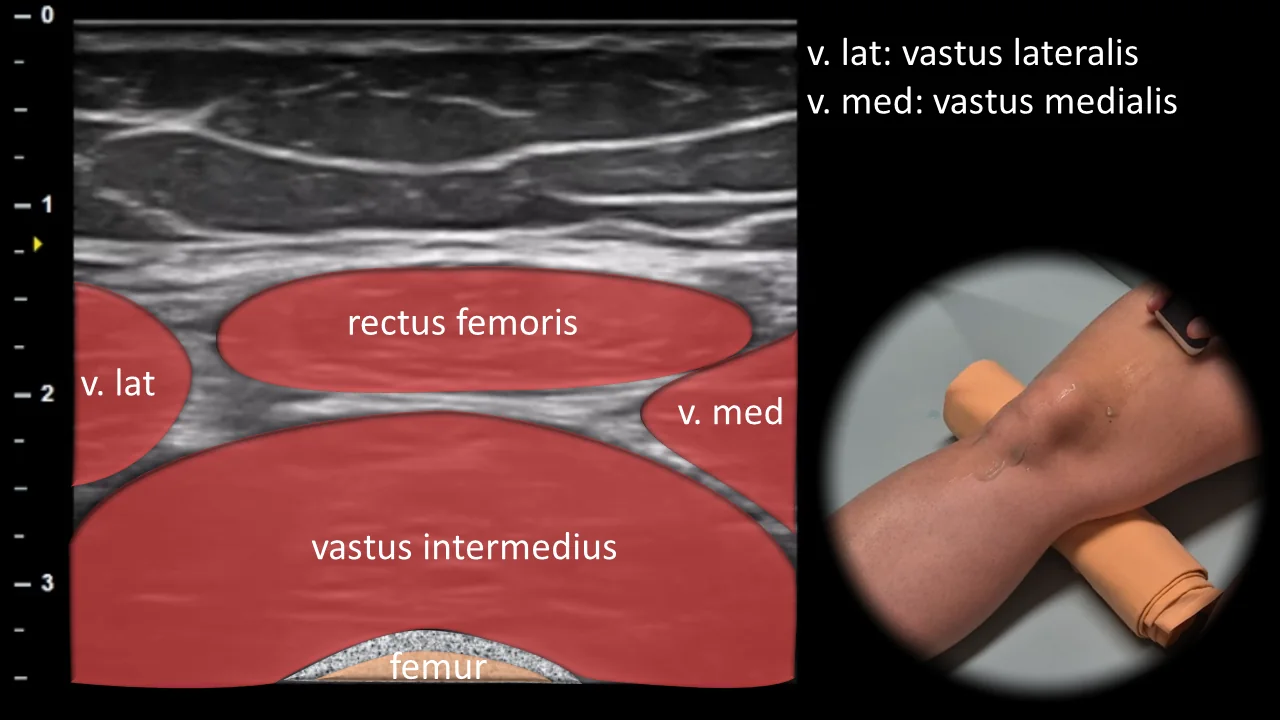
Figure 1. Ventral view, transverse plane, suprapatellar. v. lat: m. vastus lateralis, v. med: m. vastus medialis
Transverse ultrasound section of the anterior thigh at the suprapatellar level showing individual parts of the m. quadriceps femoris. Superficially in the midline, the m. rectus femoris is visible, with m. vastus lateralis and m. vastus medialis on its sides, and deeper the m. vastus intermedius, which lies against the anterior contour of the femur. The femur is displayed as a curved hyperechoic cortical line with dorsal acoustic shadowing. This projection is important for evaluating the anatomical arrangement of the quadriceps muscles, detecting muscle injuries, and providing orientation for subsequent tracking distally toward the quadriceps tendon.
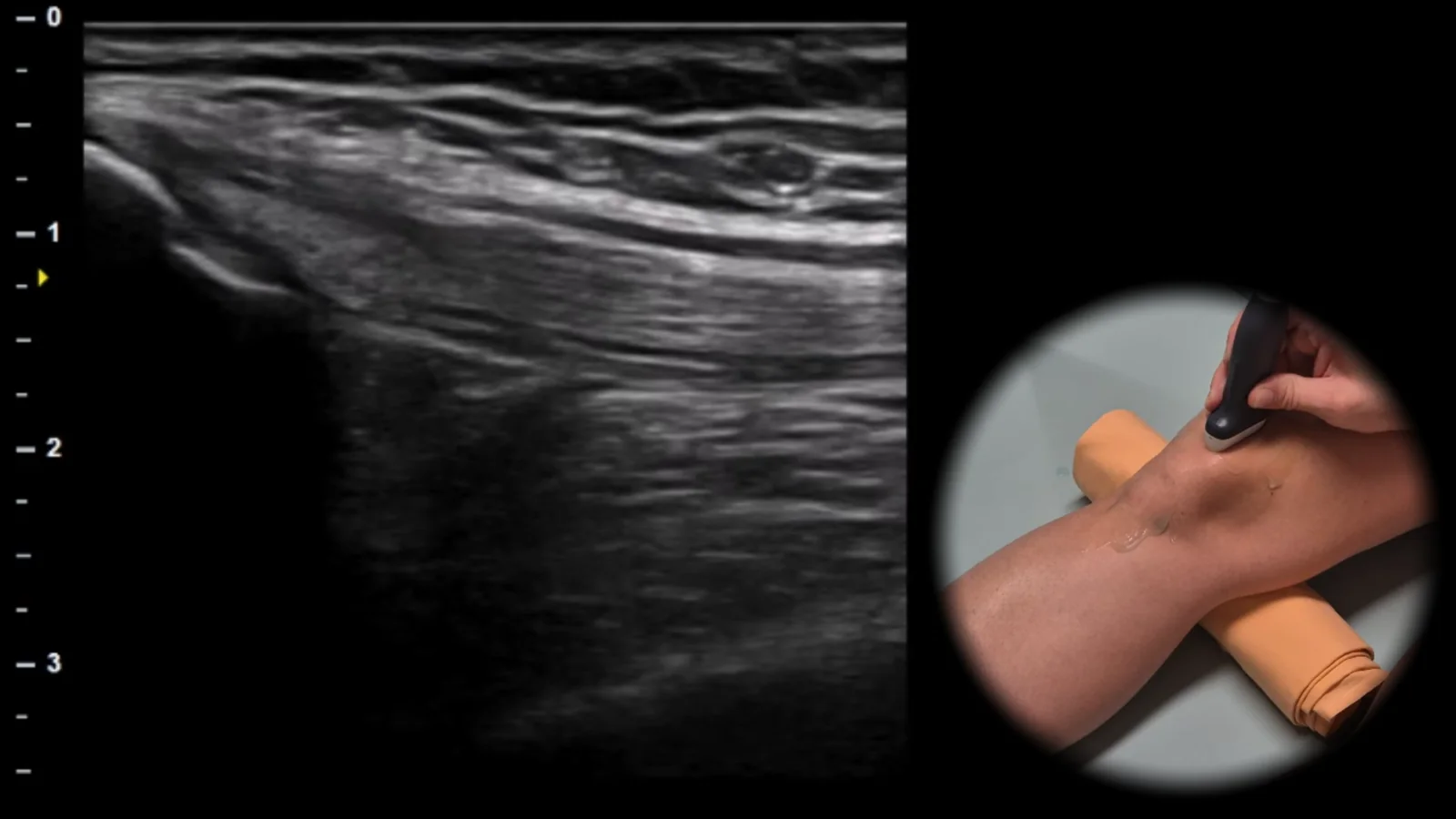
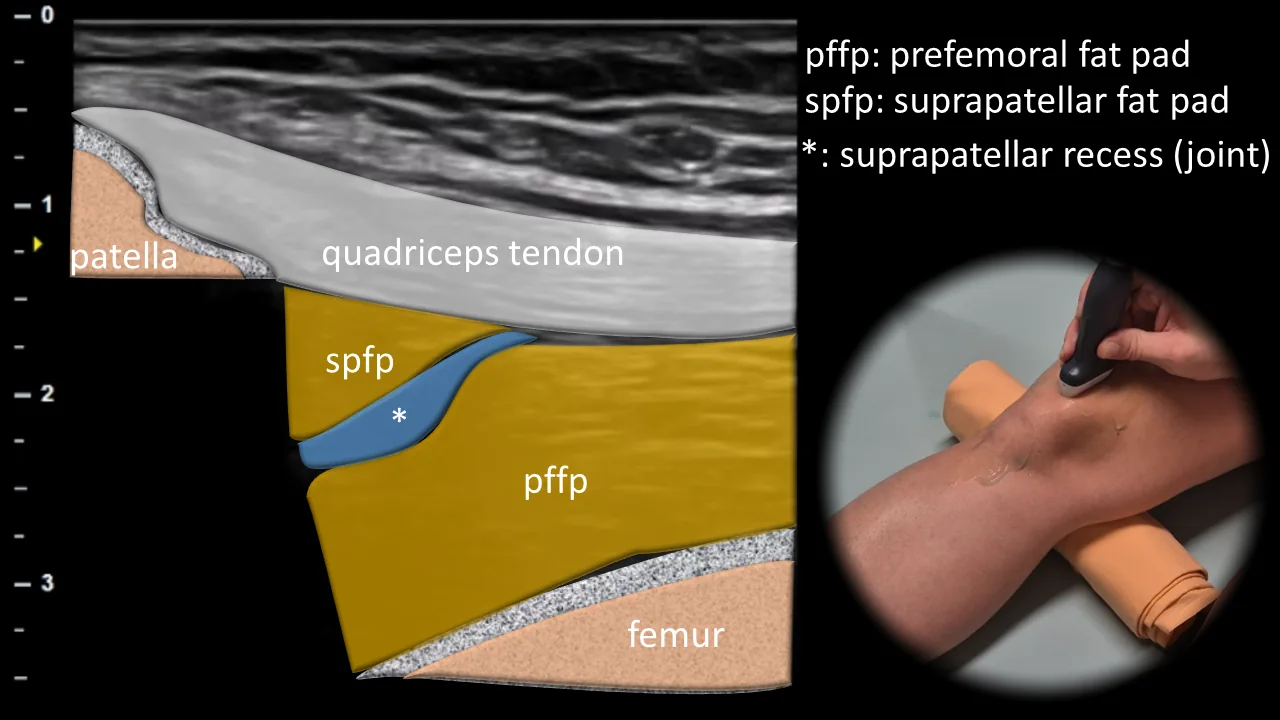
Figure 2. Ventral view, sagittal plane, suprapatellar. spfp: suprapatellar fat pad, pffp: prefemoral fat pad, *: suprapatellar recess
Longitudinal ultrasound section of the anterior part of the knee in the suprapatellar area. The quadriceps femoris tendon is shown in this projection as a broad hyperechoic fibrillar structure inserting on the superior pole of the patella. Deep beneath the tendon, the suprapatellar recess is visible as a potential space between the patella and femur, below which lies the prefemoral fat pad, while more superficially the suprapatellar fat pad is located, which together form important anatomical landmarks of this projection. This projection is crucial for evaluating the quadriceps tendon, suprapatellar recess, and signs of synovial pathology.
Clinical Note
In this area, fluid in the knee joint can be well detected, which accumulates in the suprapatellar recess and leads to its expansion in case of effusion.
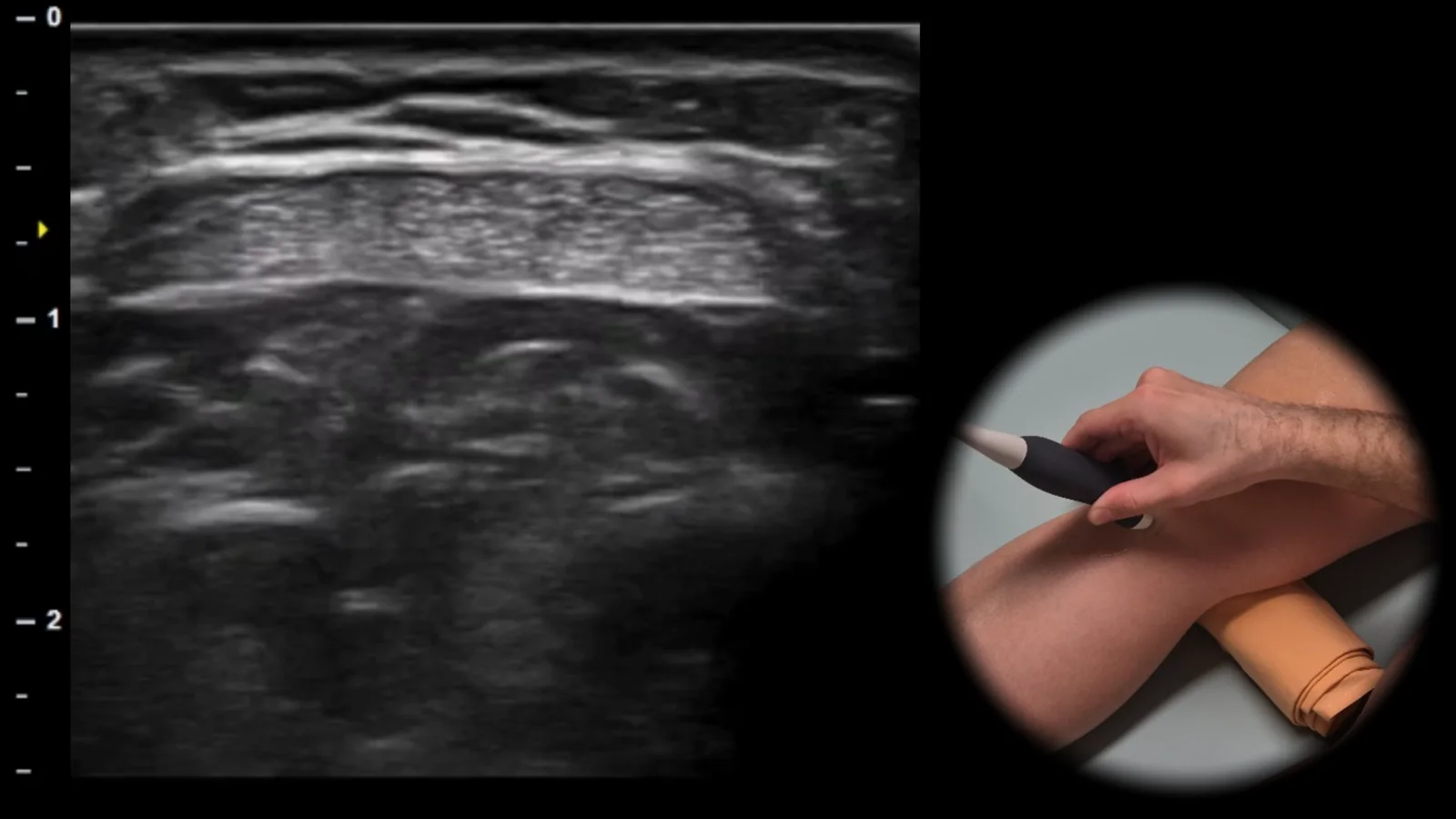
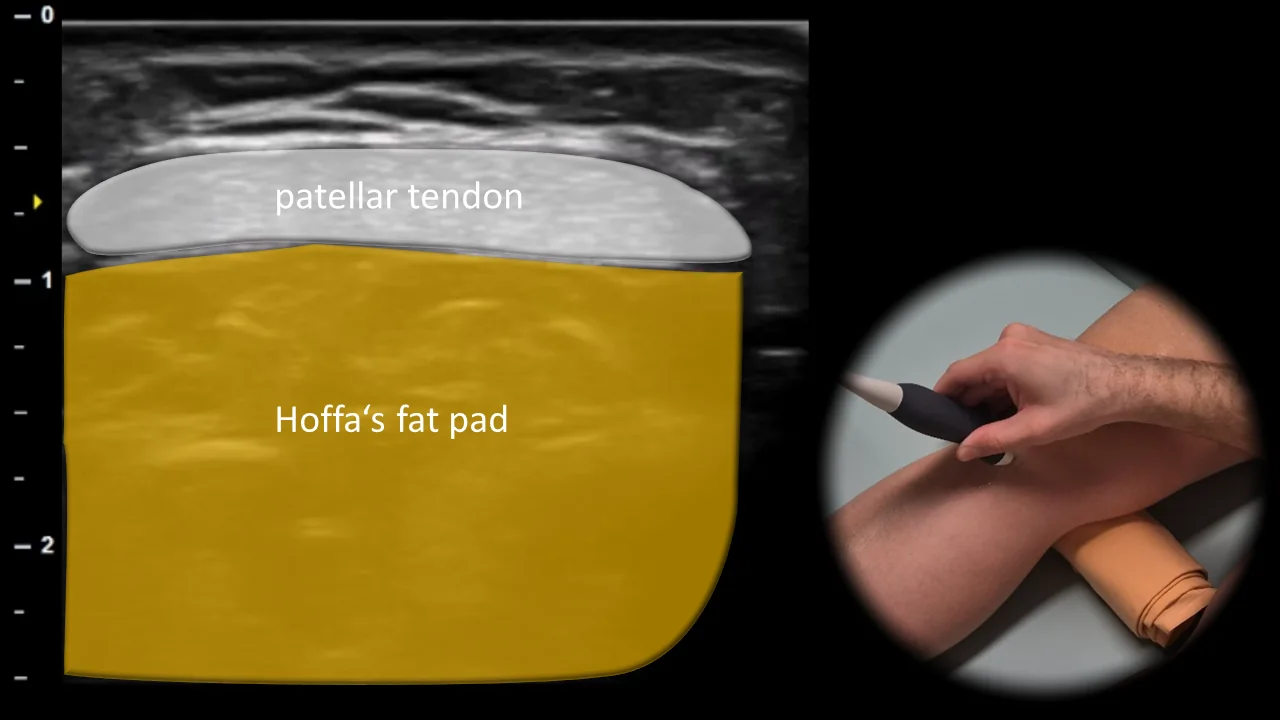
Figure 3. Ventral view, transverse plane, infrapatellar.
Transverse ultrasound section of the anterior part of the knee in the infrapatellar area. The patellar tendon is displayed in this projection as a hyperechoic fibrillar structure, beneath which Hoffa's fat pad is visible as an inhomogeneous soft tissue structure filling the anterior infrapatellar space. This projection is essential for assessment of the patellar tendon, detection of patellar tendinopathy, partial lesions, and changes in Hoffa's fat pad related to impingement or postoperative conditions.
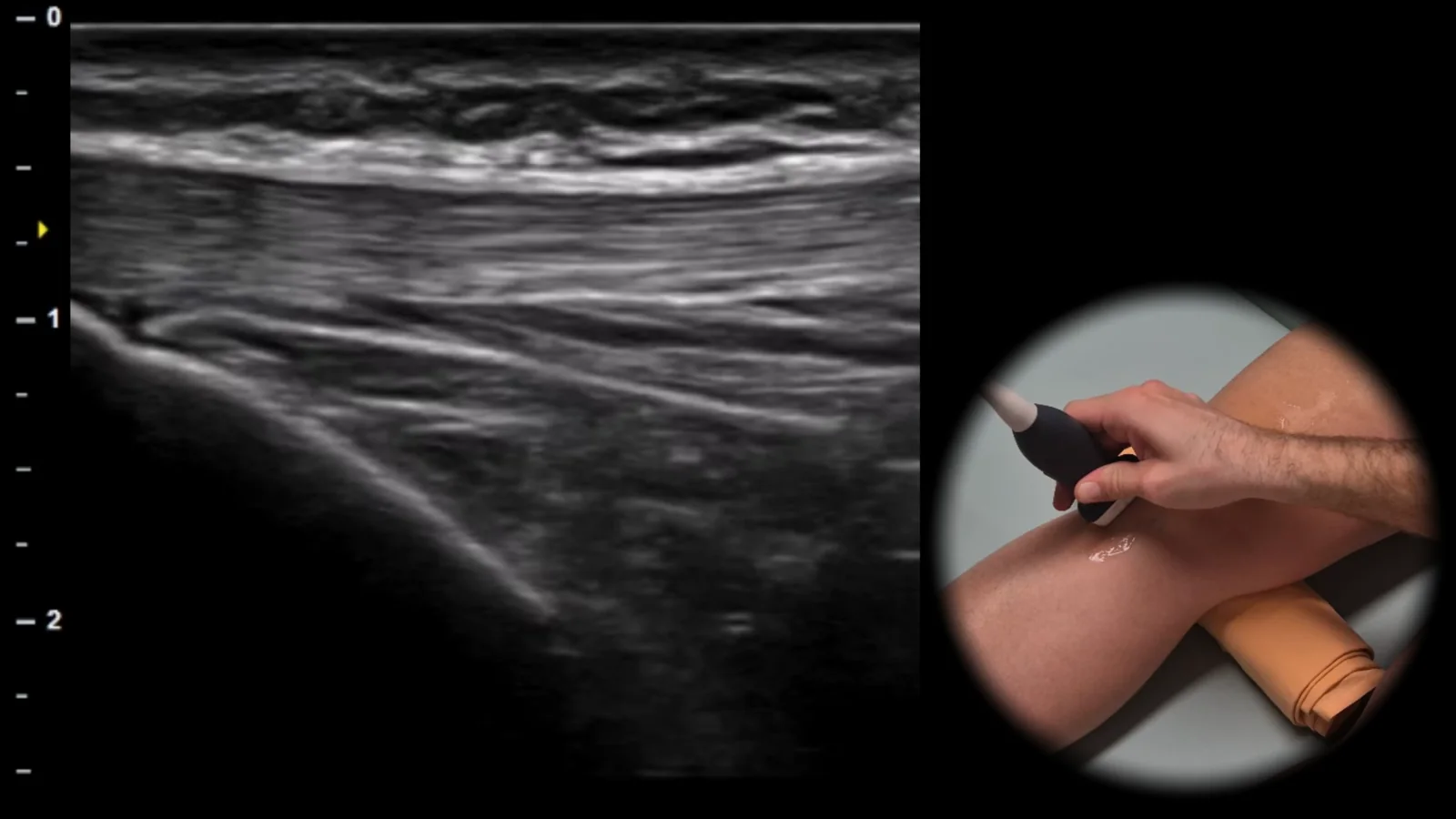
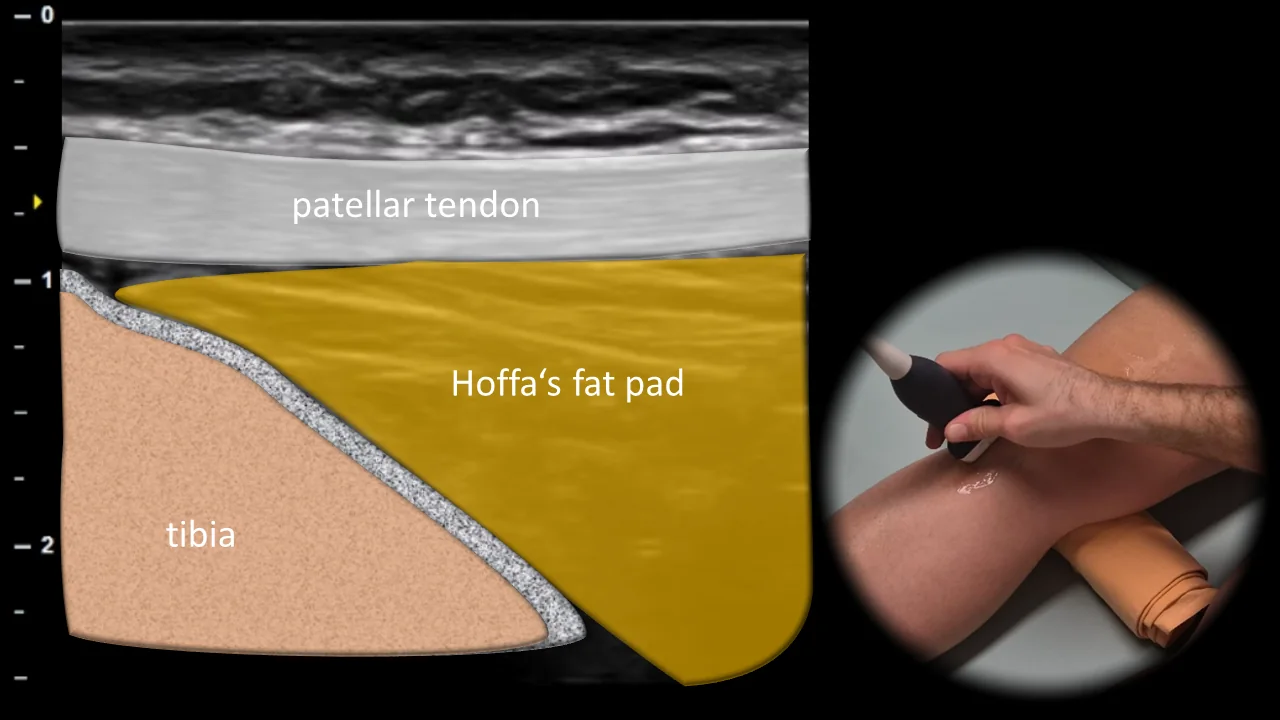
Figure 4. Ventral view, sagittal plane, infrapatellar.
Longitudinal ultrasound section of the anterior part of the knee in the infrapatellar region. The patellar tendon is displayed in this projection as a thick hyperechoic fibrillar band extending from the lower pole of the patella to its insertion on the anterior surface of the proximal tibia. Immediately below the tendon and in front of the tibia, Hoffa's fat pad is visible, which forms an important anatomical landmark of this region. This projection is essential for evaluating patellar tendinopathy, partial ruptures, and pathological changes in the area of the tibial insertion of the patellar tendon as well as Hoffa's fat pad.
2. Medial View
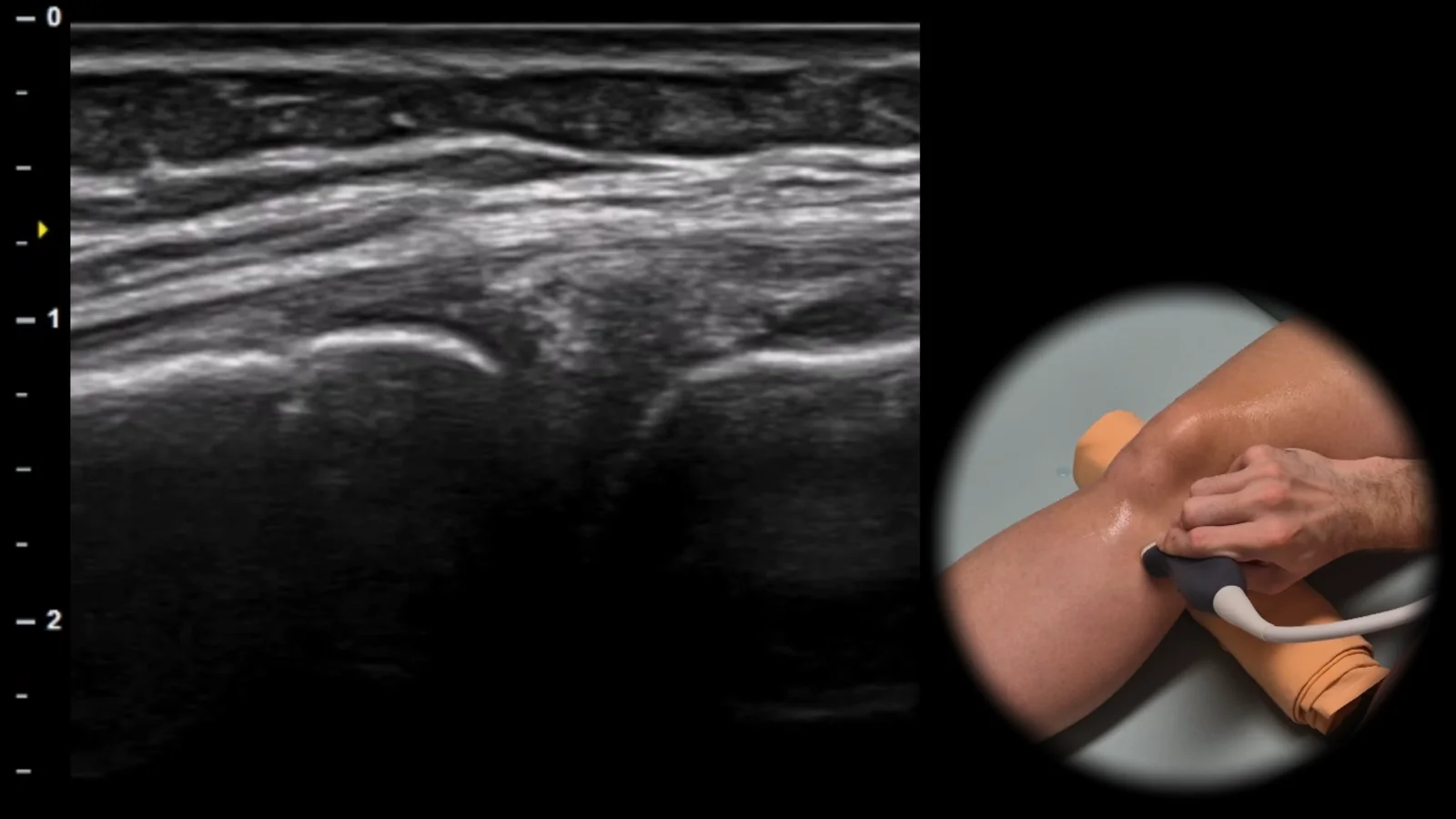
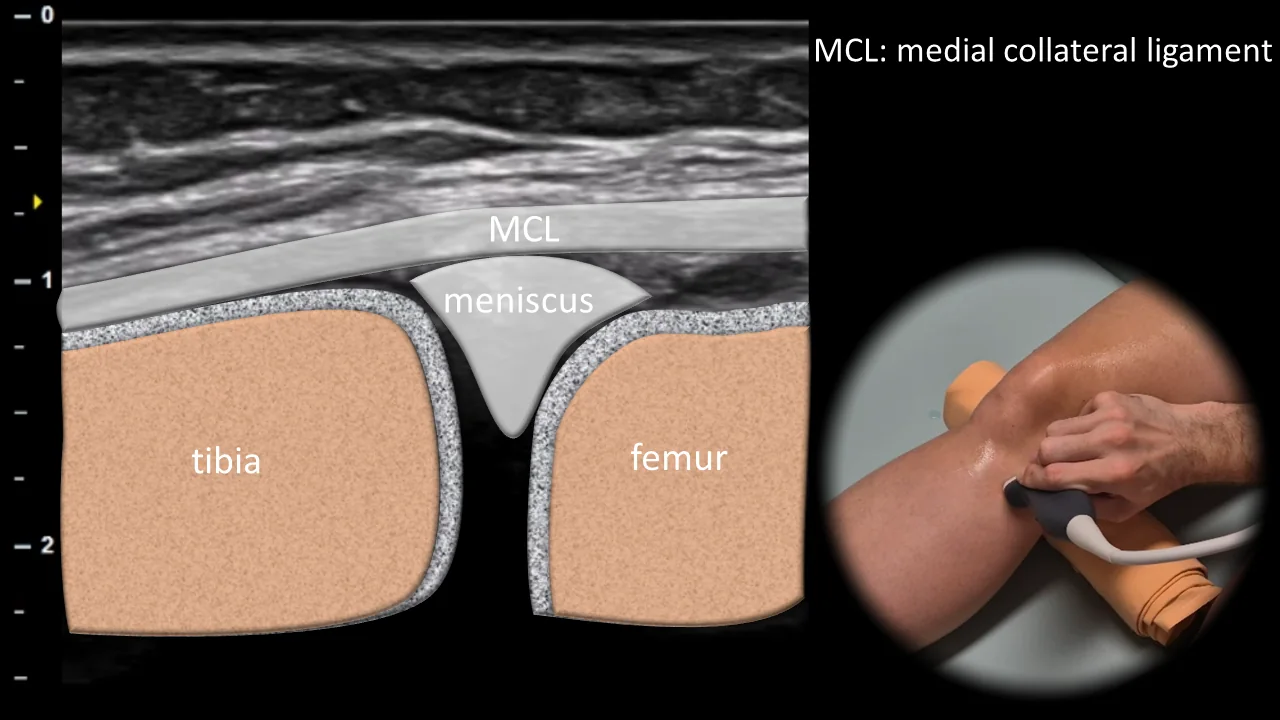
Figure 5. Medial view, frontal plane. MCL: medial collateral ligament
Longitudinal ultrasound section of the medial side of the knee showing the medial collateral ligament (MCL) as a thin, well-defined hyperechoic fibrillar band running between the femur and tibia. At the level of the joint space, the medial meniscus is visible beneath the ligament as a triangular structure positioned between the bony contours of the femur and tibia, which appear as hyperechoic cortical lines with dorsal acoustic shadowing. This projection is essential for assessing MCL integrity, detecting medial meniscus extrusion, and evaluating effusion or capsular abnormalities in the medial recess.
3. Lateral View
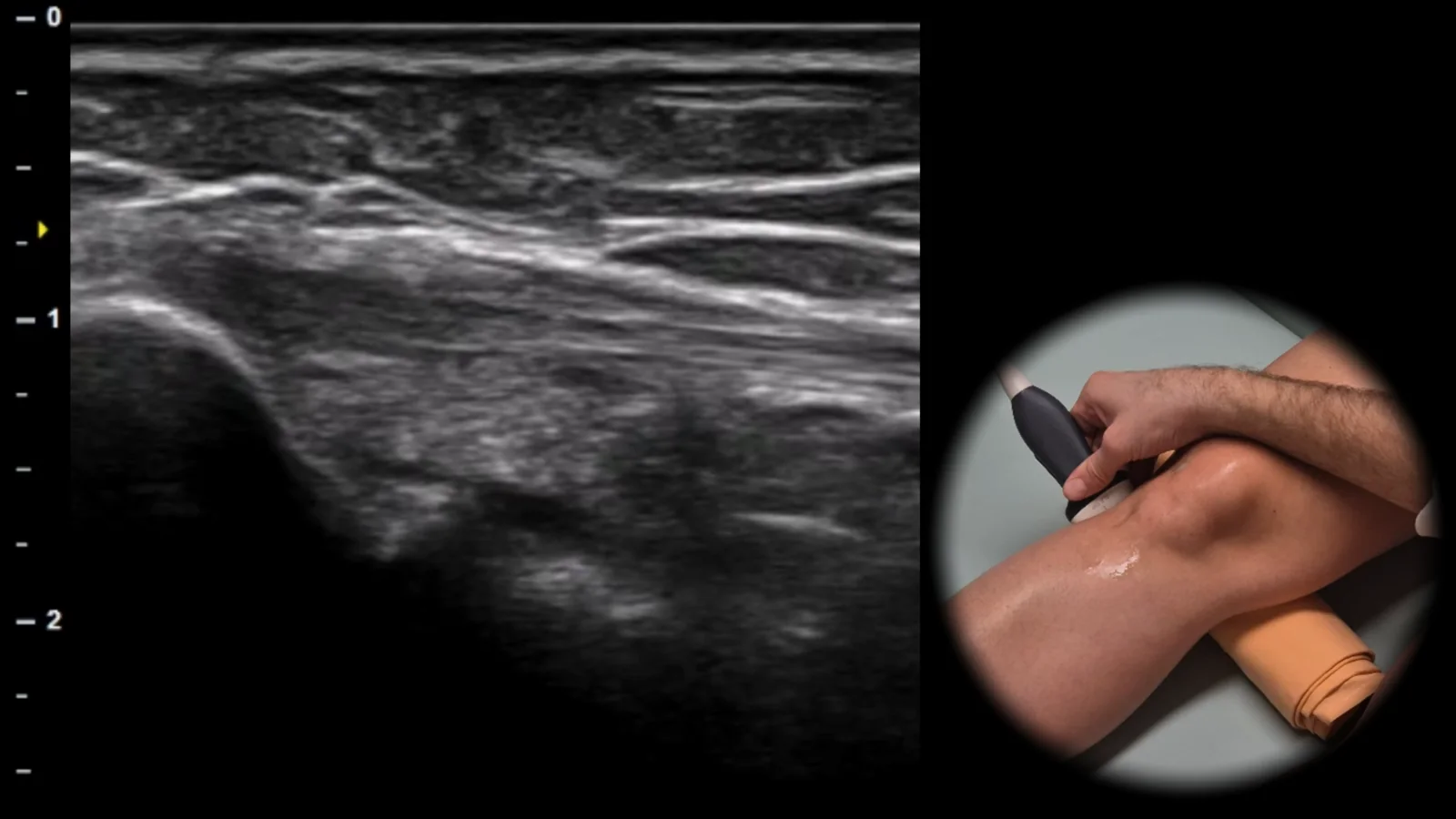
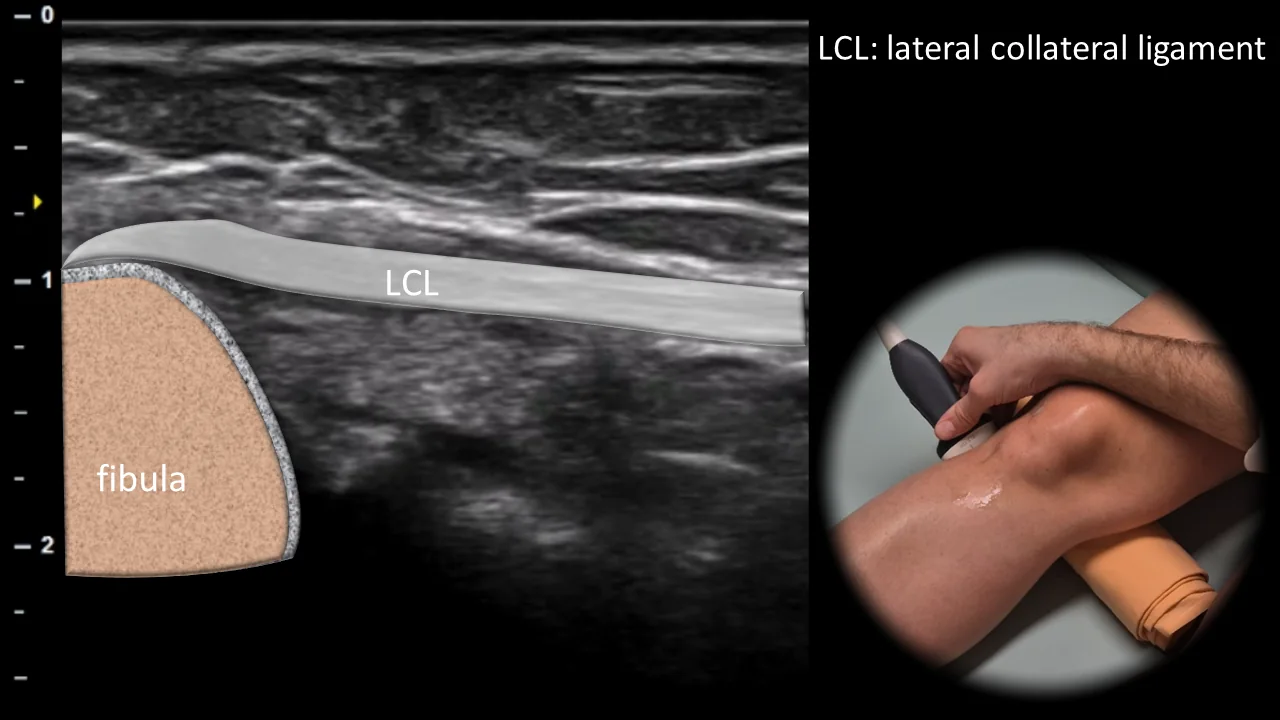
Figure 6. Lateral view, frontal plane. LCL: lateral collateral ligament
Longitudinal ultrasound section of the lateral side of the knee showing the lateral collateral ligament (LCL) as a thin hyperechoic fibrillar structure running from the lateral epicondyle of the femur to its insertion on the fibular head. The fibula is visible in this projection as the main bony landmark with a hyperechoic cortical line and posterior acoustic shadowing. This projection is essential for assessing LCL integrity and for detecting enthesopathy, partial ruptures, or avulsion injuries in the area of the fibular insertion.
4. Dorsal View
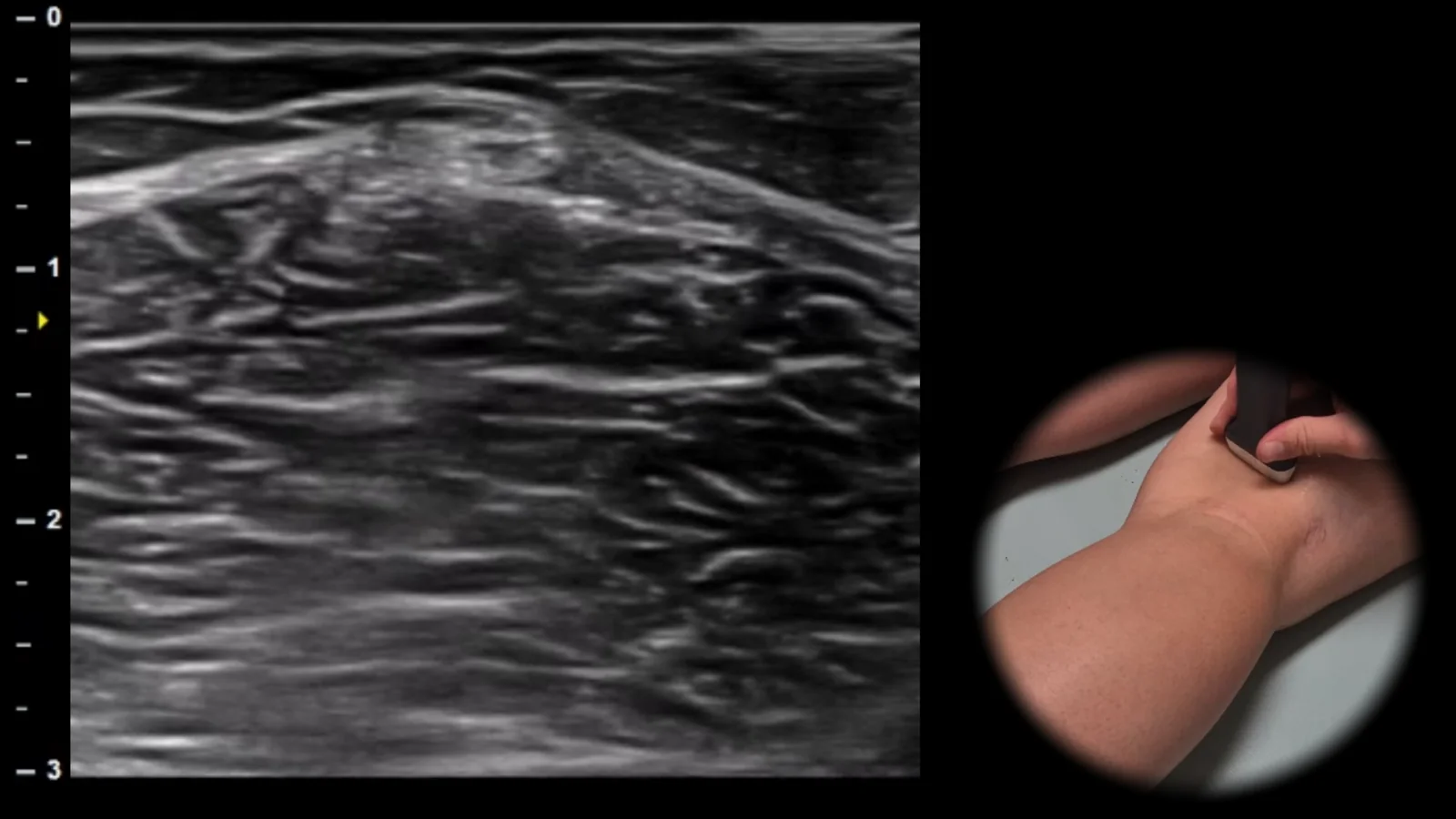
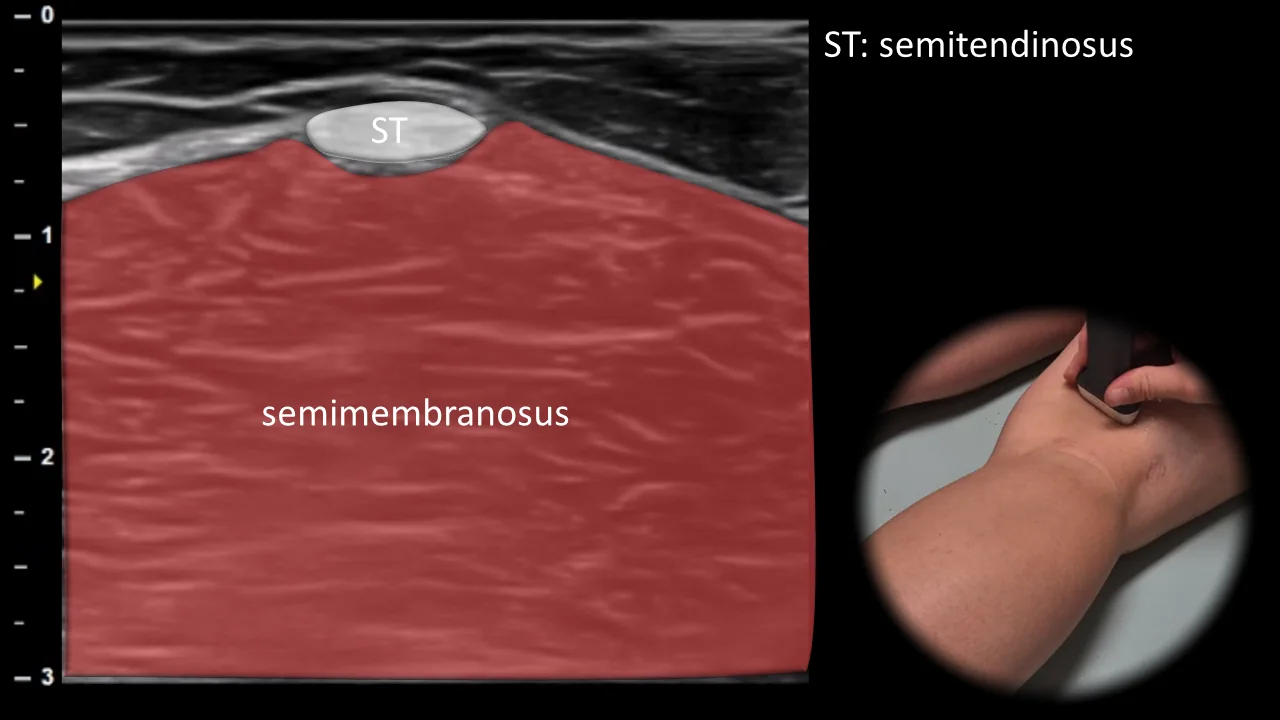
Figure 7. Dorsal view, transverse plane. ST: semitendinosus muscle tendon
Transverse ultrasound section of the posterior medial part of the knee showing the semitendinosus muscle tendon (ST) as an oval structure positioned superficially on the semimembranosus muscle, which forms the broader muscular base of this projection. This typical spatial arrangement allows clear identification of the medial portion of the hamstrings in the popliteal area. This projection is important as a reference point for tracking the medial hamstrings and for evaluating their tendinous and muscular lesions. Clinical note: the characteristic appearance referred to as "cherry on cake" facilitates rapid sonographic orientation and localization of the semitendinosus muscle tendon.
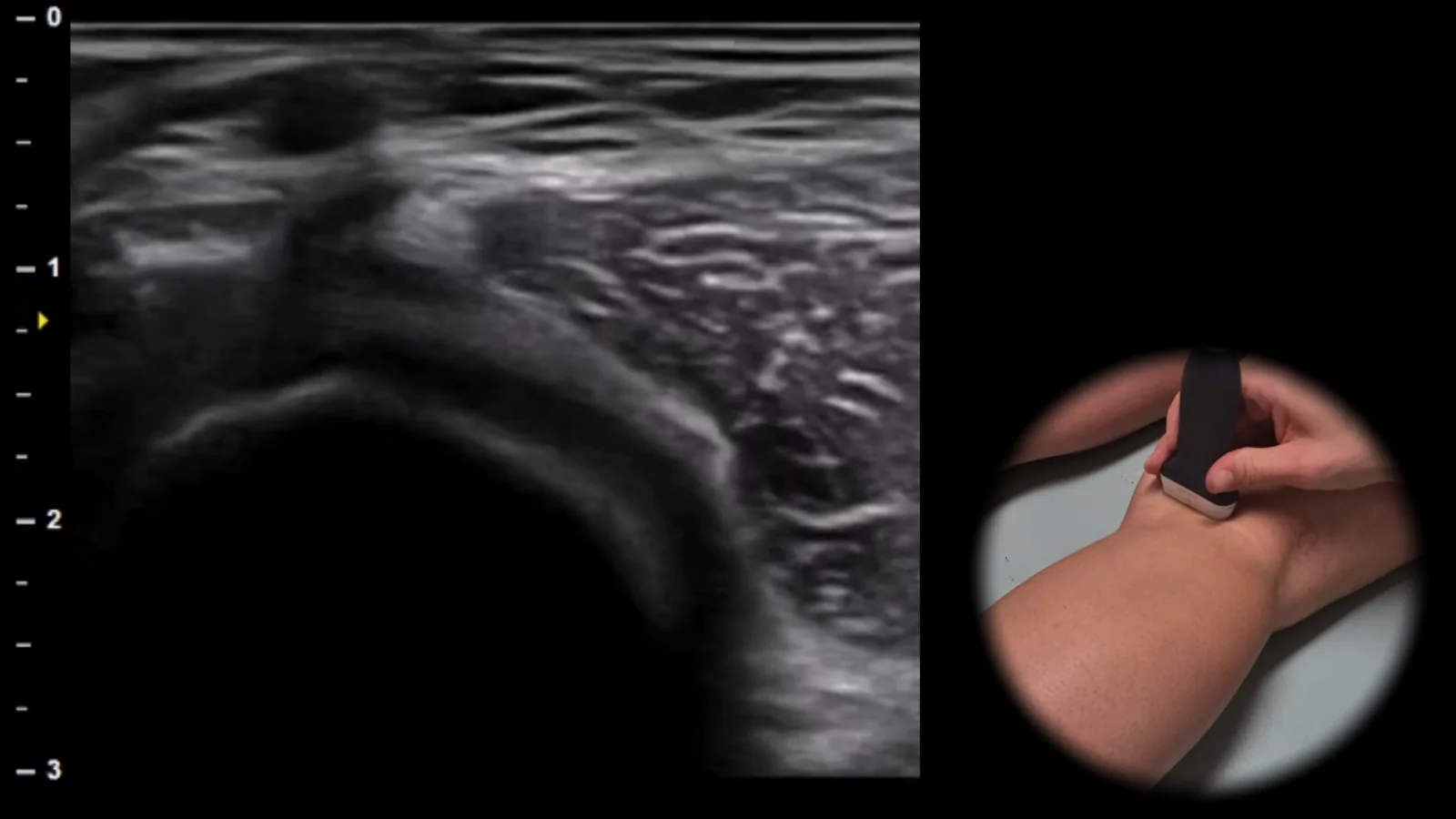
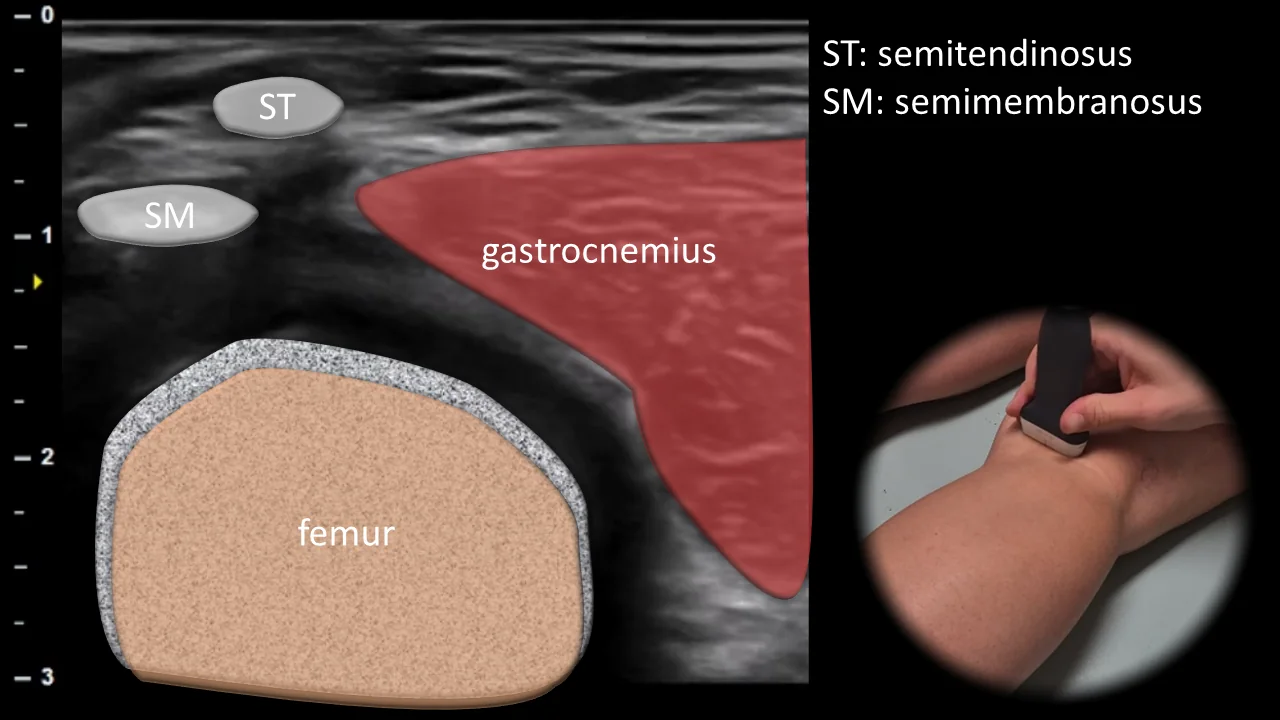
Figure 8. Dorsal view, transverse plane. SM: semimembranosus muscle tendon, ST: semitendinosus muscle tendon
Transverse ultrasound section of the posterior medial part of the knee showing the area between the semimembranosus muscle tendon (SM) and the medial head of the gastrocnemius muscle. In this projection, the semitendinosus muscle tendon (ST) is also visible, along with the deep bony contour of the femur as the main anatomical landmark. This projection is essential for evaluating the popliteal region and particularly for detecting Baker's cyst, which typically appears as a fluid collection between the semimembranosus muscle tendon and the medial head of the gastrocnemius muscle.
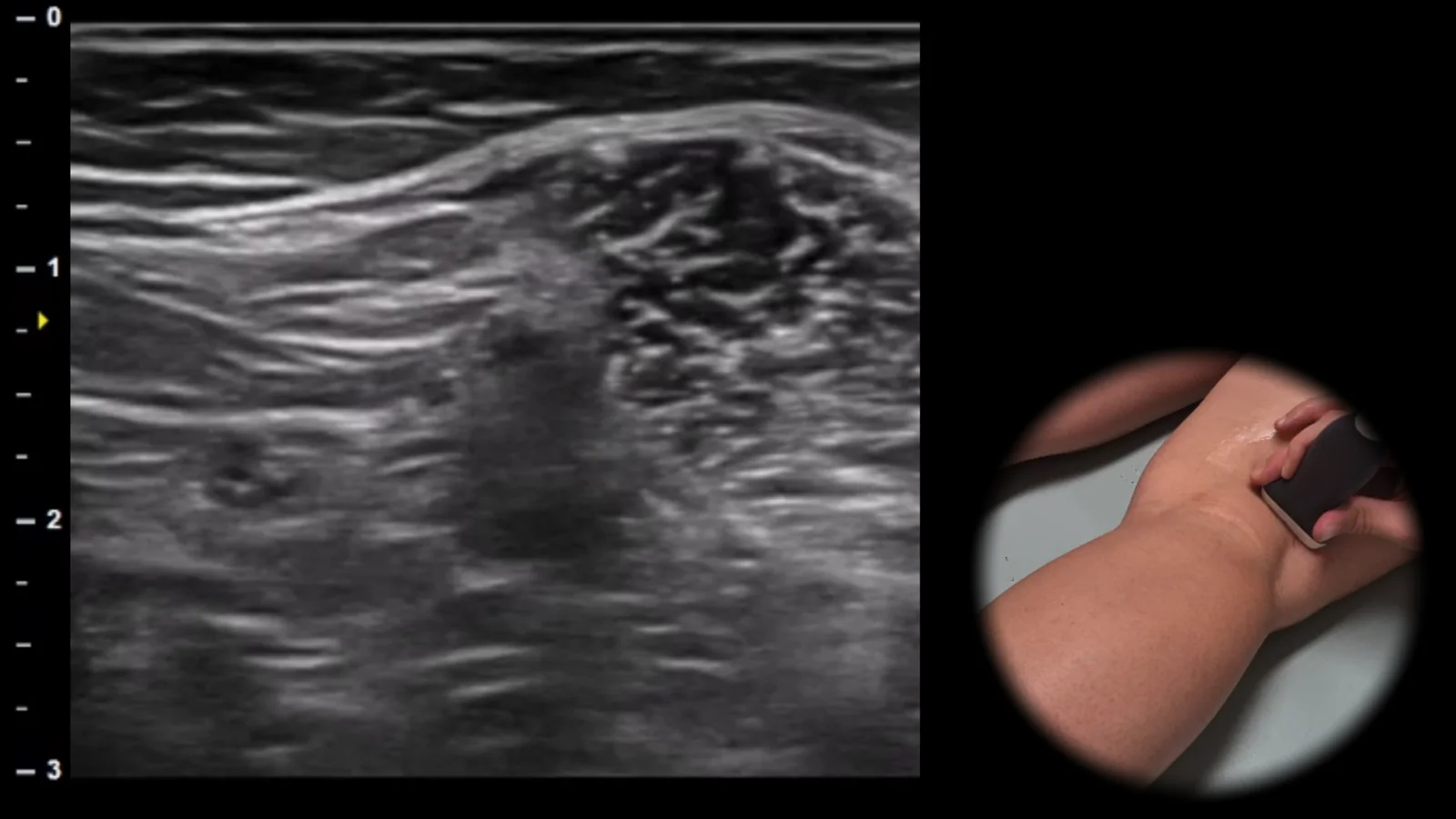
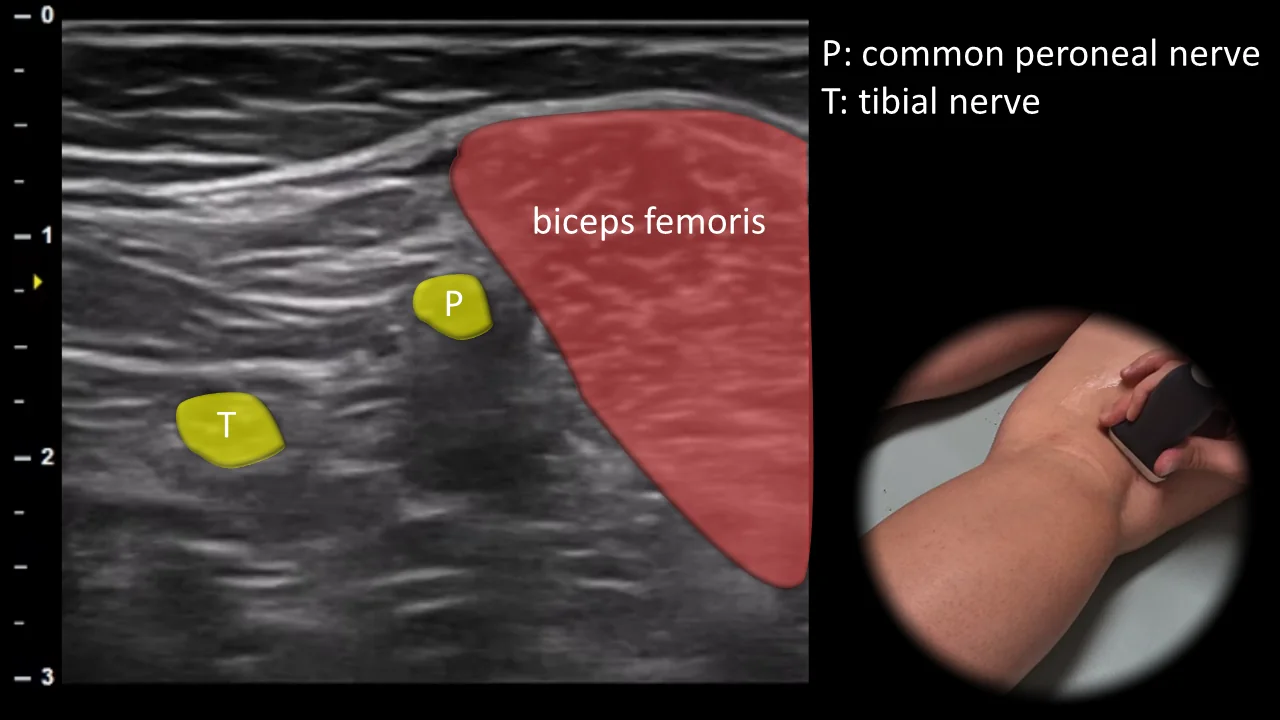
Figure 9. Dorsal view, transverse plane. T: tibial nerve, P: common fibular nerve
Transverse ultrasound section of the posterolateral part of the knee in the popliteal fossa region. In this projection, the biceps femoris muscle is visible as an important muscular landmark, near which the common fibular nerve (P) can be visualized as an oval structure with typical fascicular appearance, branching laterally, while the tibial nerve (T) continues more medially. This projection is crucial for evaluating sciatic nerve bifurcation and for detecting entrapment, compression, or traumatic injury of peripheral nerves in the posterolateral knee region.
Unlock the full Health Library
Full access to scanning protocols, anatomy, and clinical references. Cancel anytime.
- Every protocol and anatomy reference
- Original ultrasound illustrations and video demonstrations
- Sync across mobile and web