Ultrasound examination
Examination protocol
Ventral view
- Transverse plane
- Sagittal plane
Dorsal view
- Transverse plane
- Sagittal plane
Dorsal view
- Transverse plane
- Sagittal plane
Interactive feature, available in the app
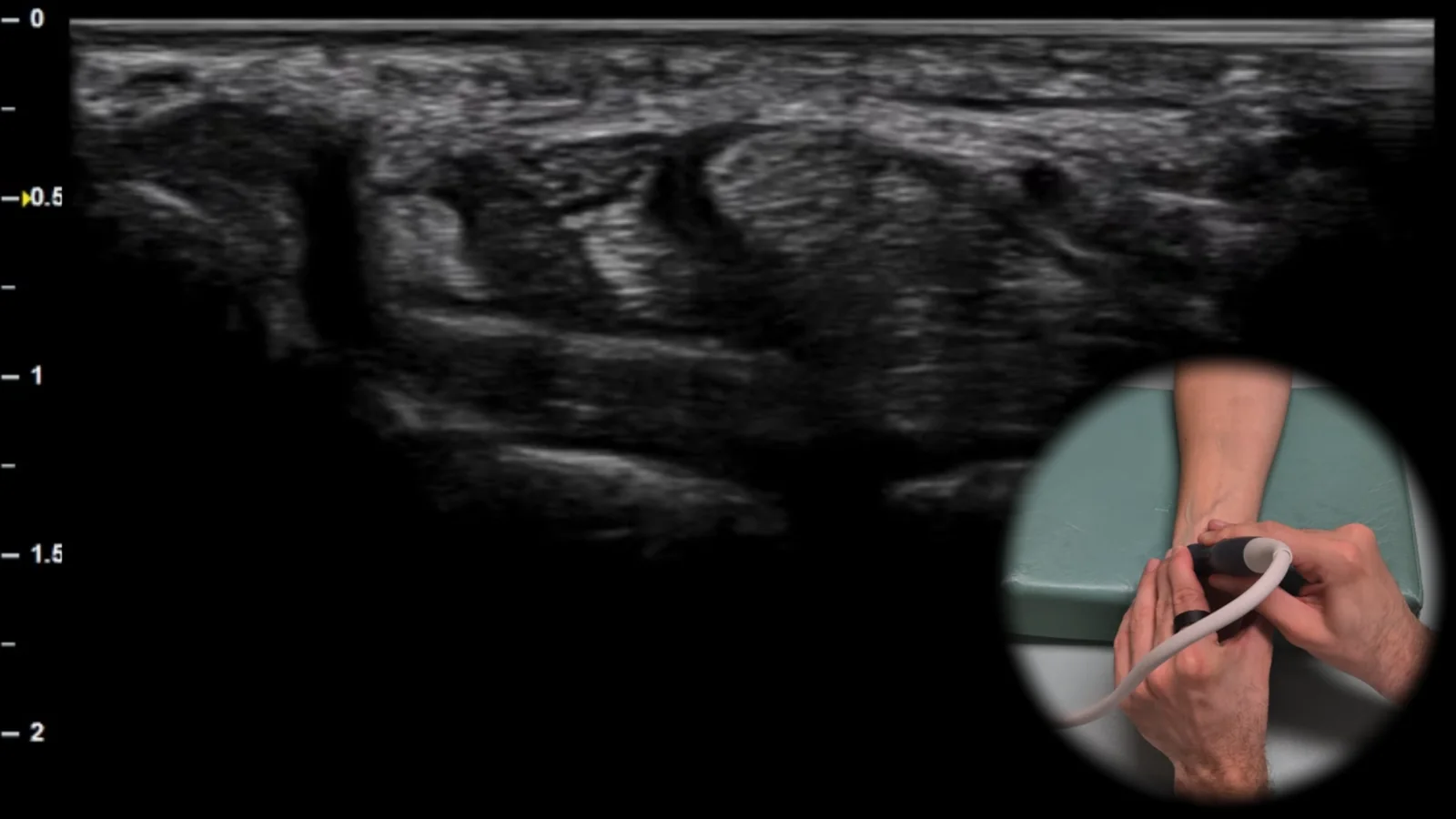
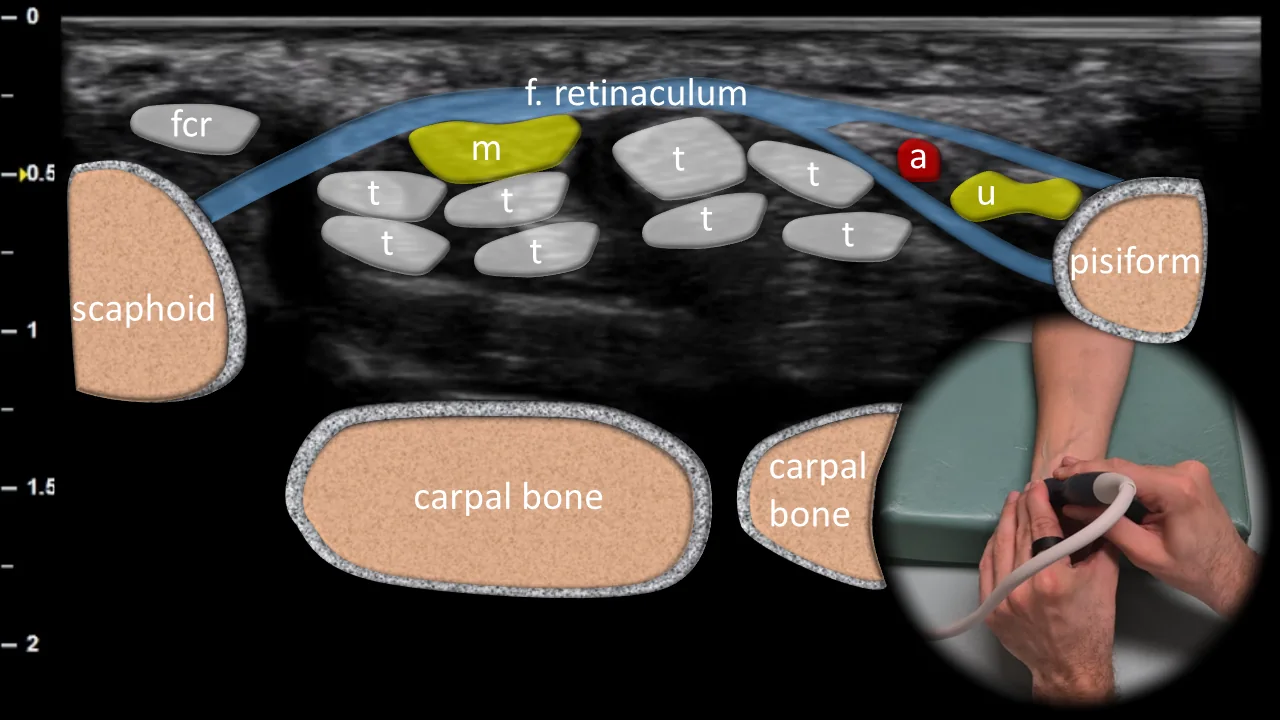
Figure 1. Ventral view, transverse plane. fcr: m. flexor carpi radialis, m: n. medianus, a: a. ulnaris, u: n. ulnaris, t: flexor tendons
Transverse ultrasound section of the volar side of the wrist at the level of the carpal tunnel and Guyon's canal. Key bony landmarks include the os scaphoideum radially and os pisiforme ulnarly, between which the flexor retinaculum can be seen overlying the flexor tendons (t) and n. medianus (m) in the carpal tunnel region. Ulnar to this area, the a. ulnaris (a) and n. ulnaris (u) are visible as they pass through Guyon's canal, while radially the tendon of m. flexor carpi radialis (fcr) is shown. This projection is essential for evaluating compressive neuropathies of the n. medianus and n. ulnaris, as well as for detecting flexor tenosynovitis and the presence of ganglion cysts in the volar wrist region.
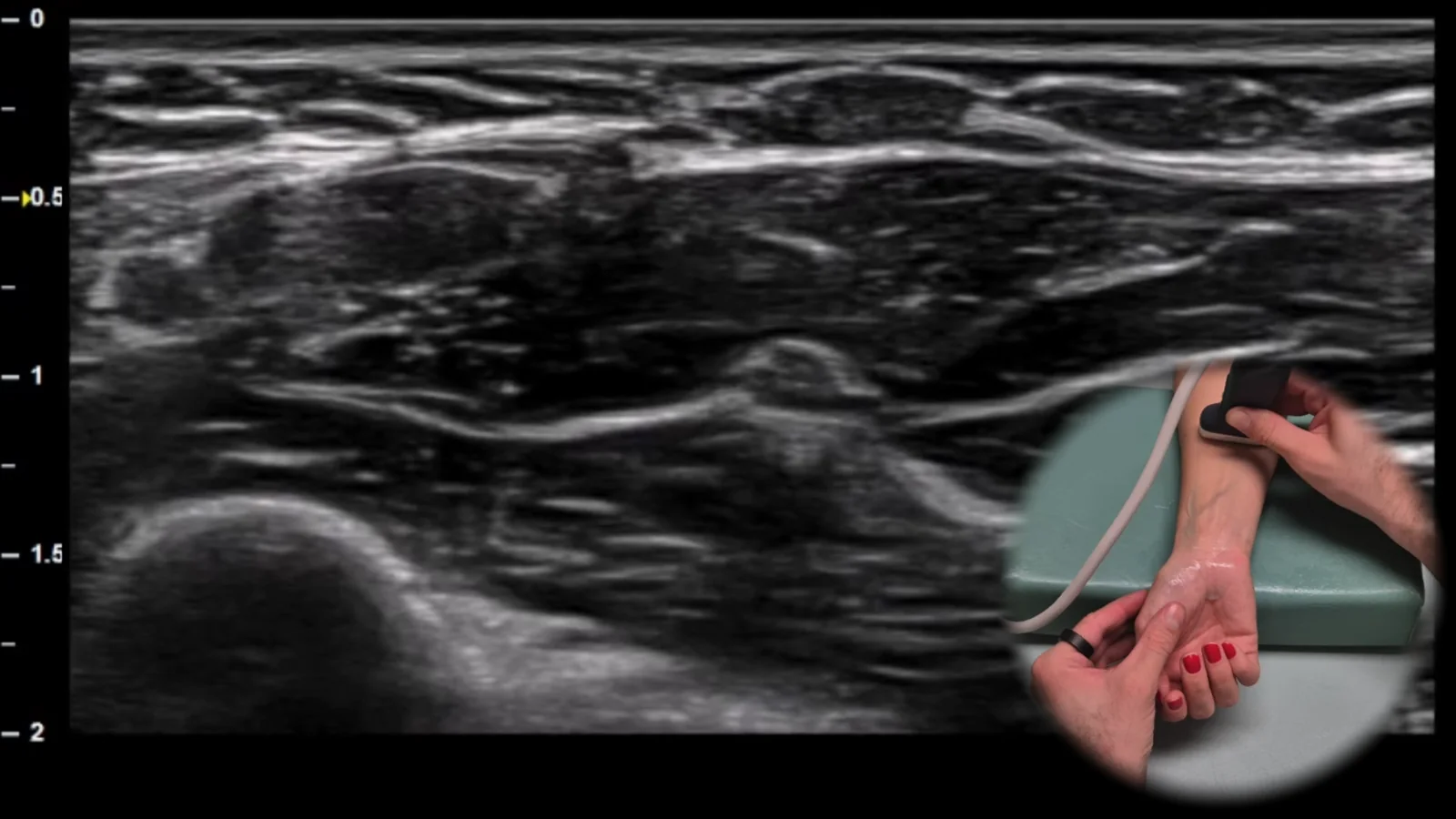
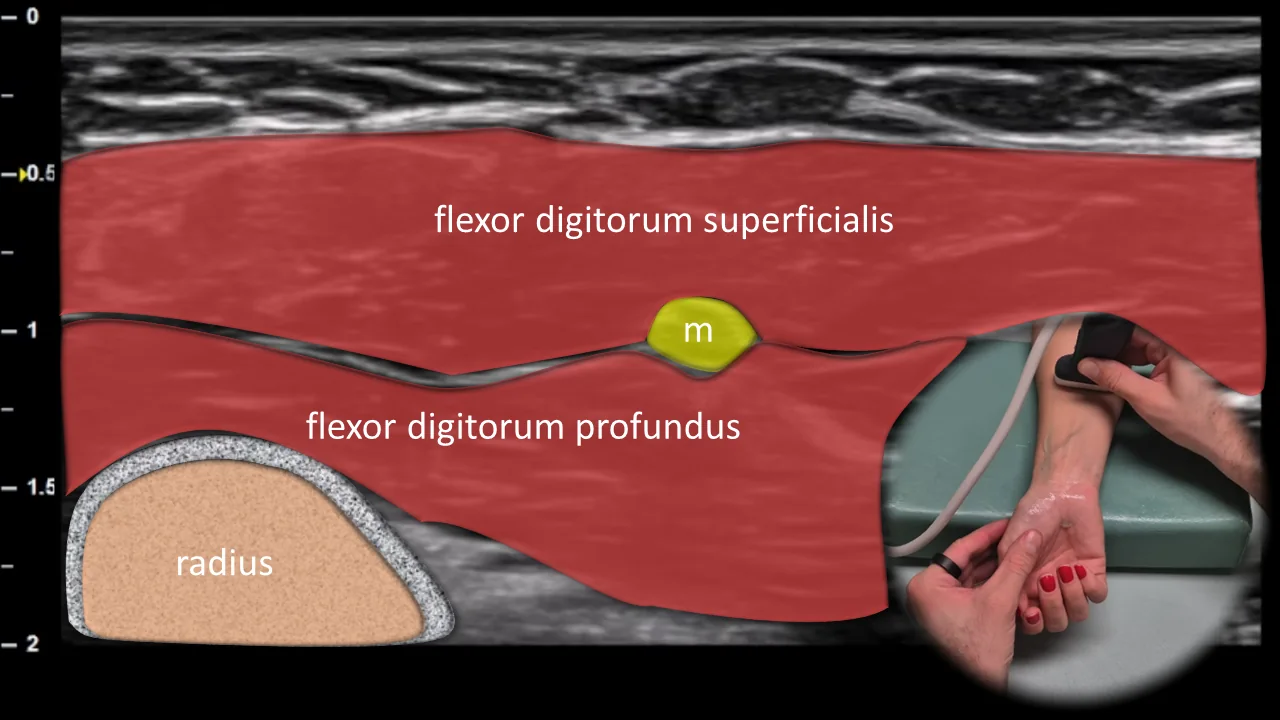
Figure 2. Ventral view, transverse plane. m: median nerve
Transverse ultrasound section of the volar aspect of the distal forearm during proximal tracking of the median nerve from the carpal tunnel area. The median nerve (m) is positioned in this projection between the flexor digitorum superficialis and flexor digitorum profundus muscles, with the radius visible deeper as a bony landmark. At this level, the median nerve has a typical fascicular ("honeycomb") appearance, which is important for assessing its morphology and for detecting pathological changes in compressive neuropathies or other nerve involvement.
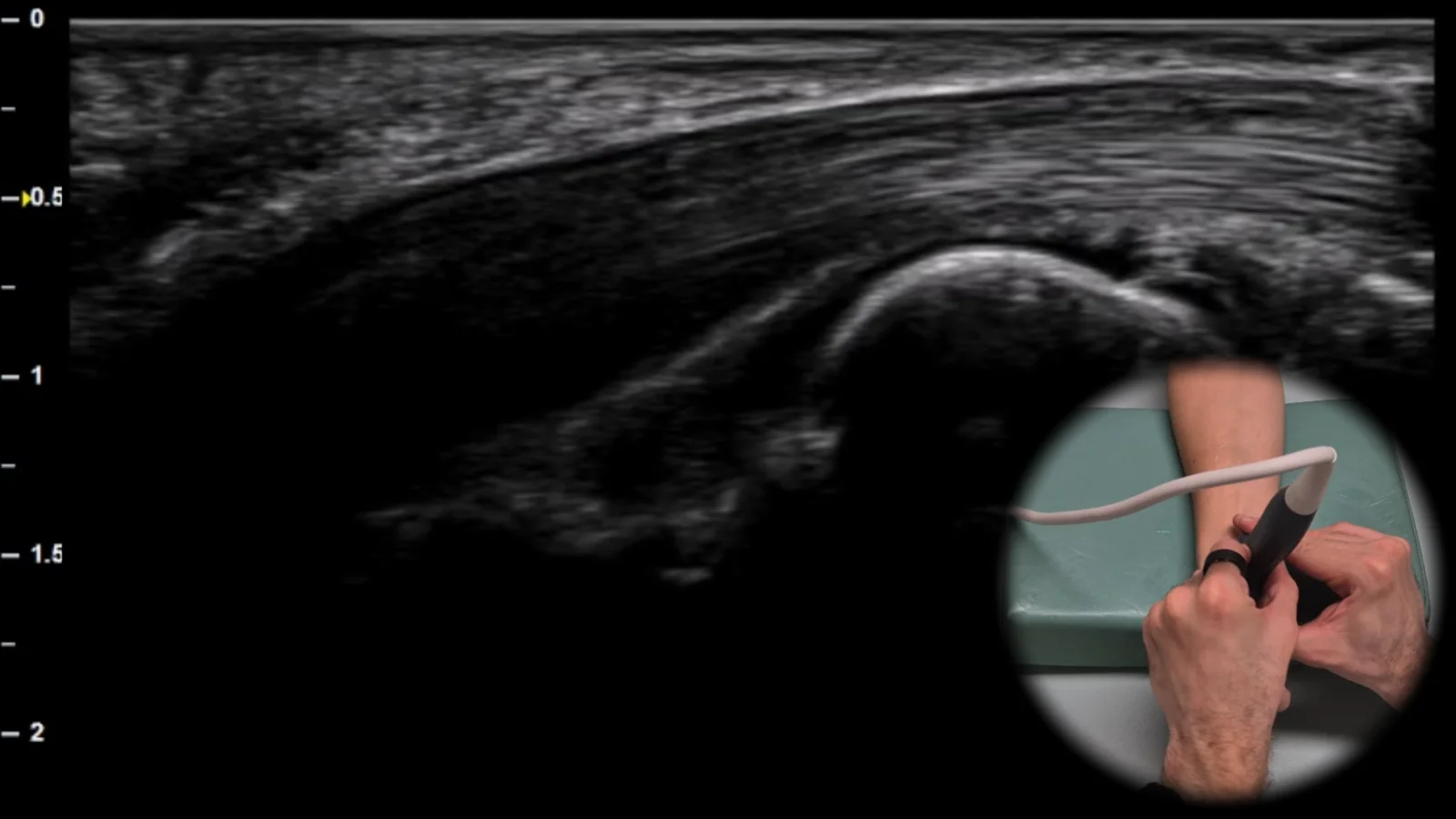
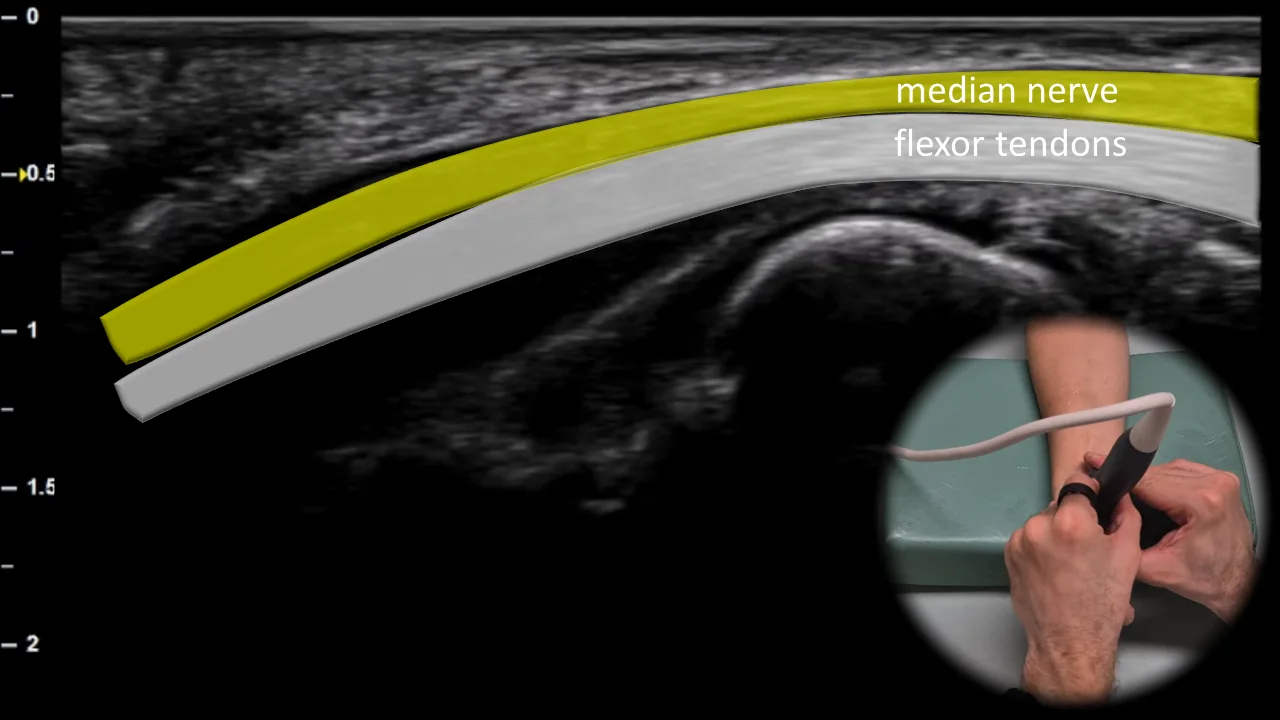
Figure 3. Ventral view, sagittal plane. m: n. medianus
Longitudinal ultrasound section of the volar side of the wrist showing the n. medianus at the entrance to the carpal tunnel. The nervus medianus (m) is visible in this projection as a striated structure with parallel echogenic lines, located superficially above the flexor tendons, which corresponds to its typical longitudinal fascicular architecture. This projection is important for assessing nerve continuity, changes in its course, and potential signs of compression at the carpal tunnel entrance.
Clinical Note
In median nerve compression, focal narrowing of the nerve with proximal dilatation may be visible at the site of entry into the carpal tunnel, which in longitudinal view resembles a "bottle neck" shape.
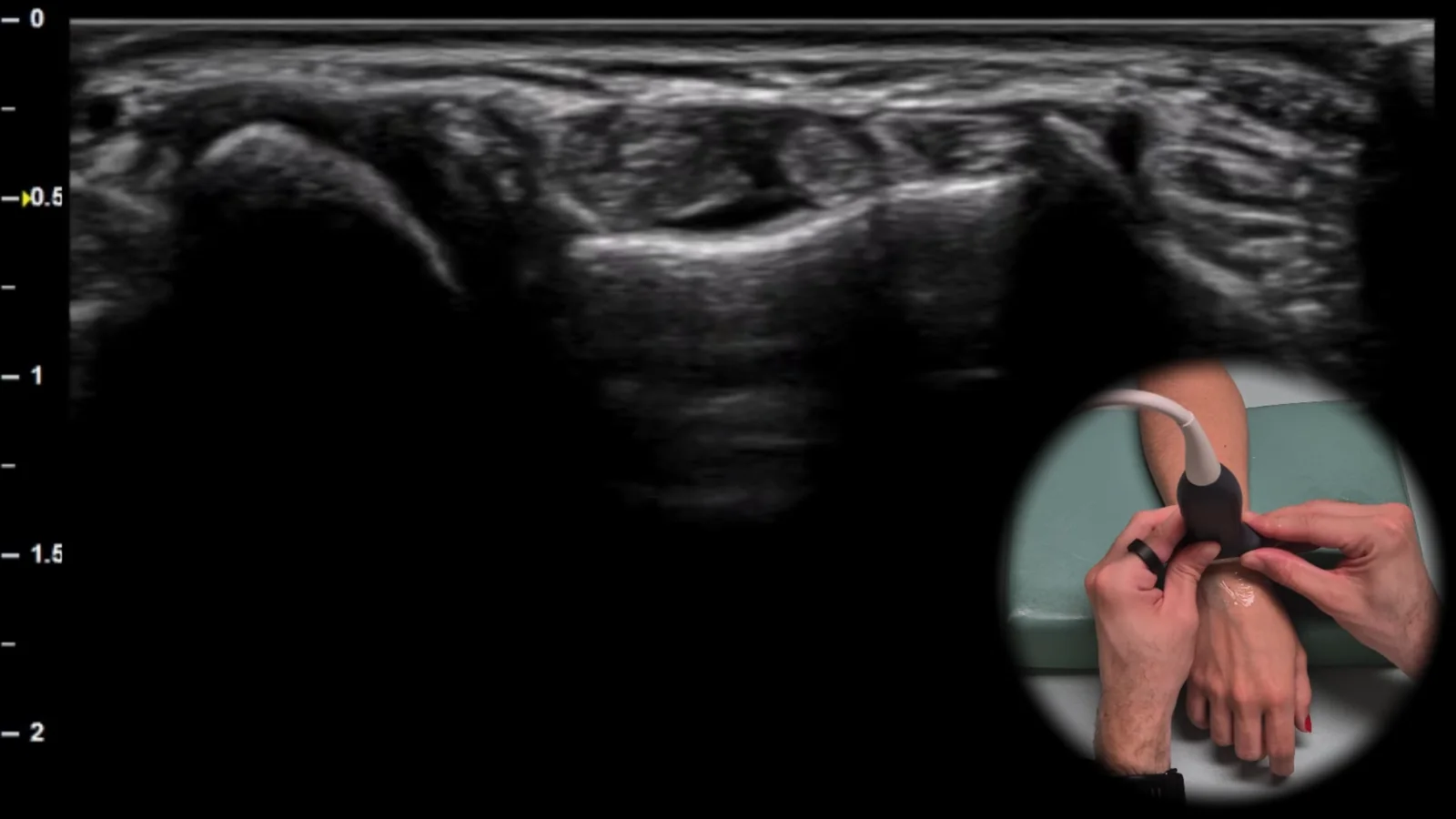
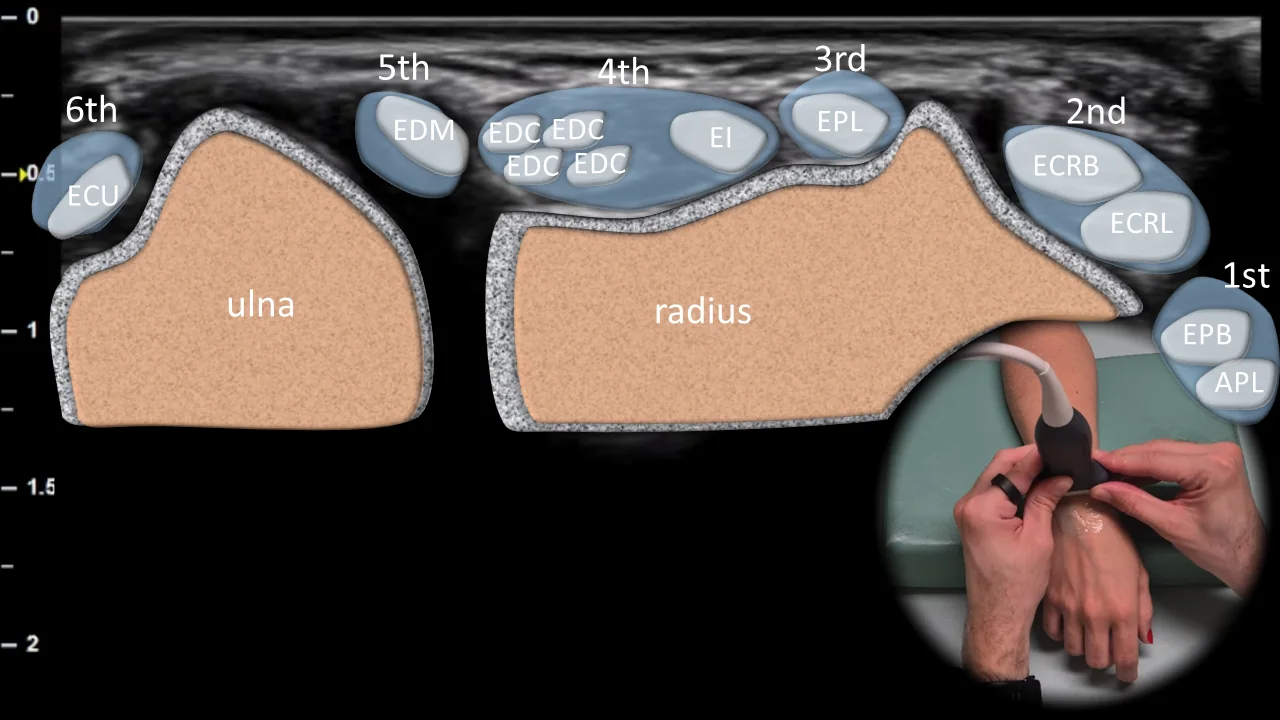
Figure 4. Dorsal view, transverse plane. ECU: m. extensor carpi ulnaris, EDM: m. extensor digiti minimi, EDC: m. extensor digitorum communis, EI: m. extensor indicis, EPL: m. extensor pollicis longus, ECRB: m. extensor carpi radialis brevis, ECRL: m. extensor carpi radialis longus, EPB: m. extensor pollicis brevis, APL: m. abductor pollicis longus
Transverse ultrasound section of the dorsal aspect of the wrist at the level of the distal radius. In this projection, all six extensor compartments can be clearly visualized, from the ulnarly located tendon of the m. extensor carpi ulnaris to the radially located tendons of the first compartment, particularly the m. abductor pollicis longus and m. extensor pollicis brevis; between them, the tendons of other extensors running over the distal radius and ulna are also visible. This projection is essential for the orientation assessment of extensor compartments and for the detection of tenosynovitis, subluxations, and degenerative changes of tendons in the dorsal wrist area.
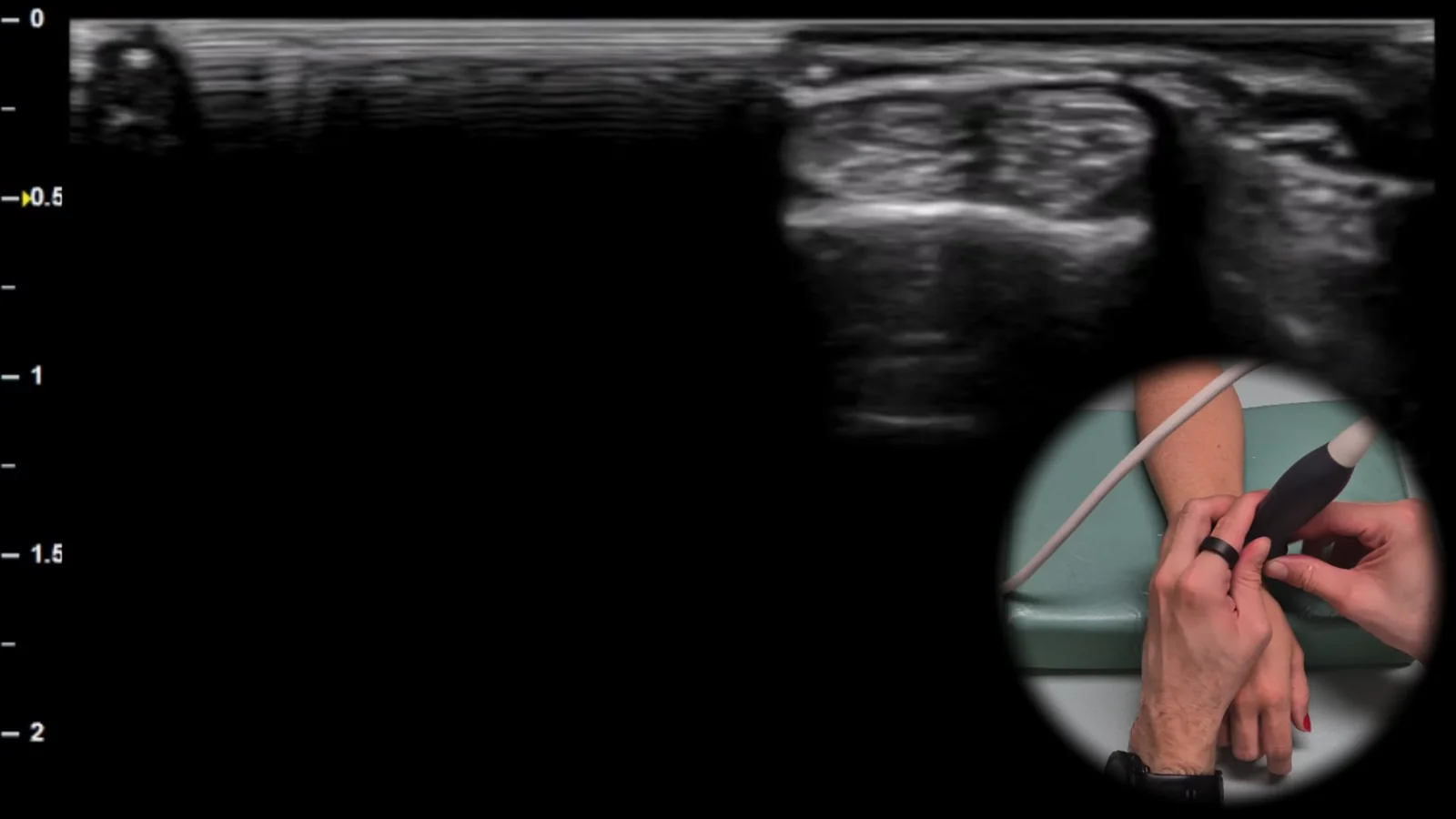
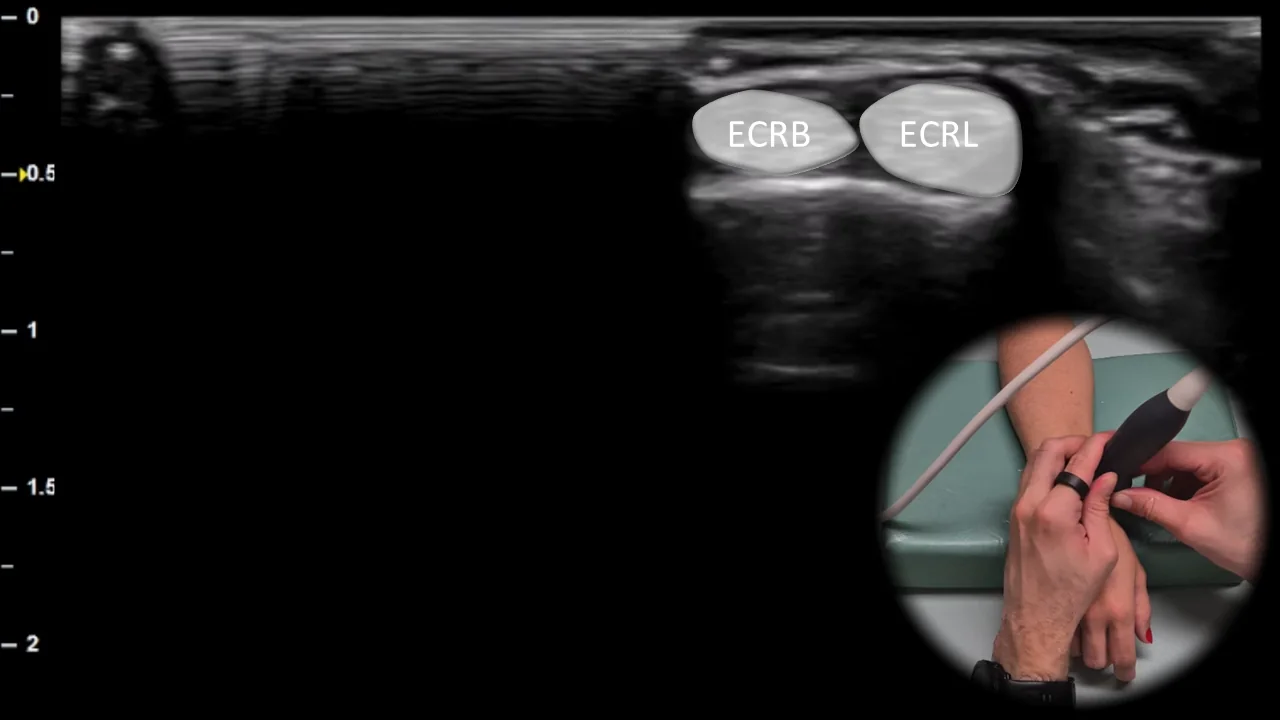
Figure 5. Dorsal view, transverse plane. ECRB: m. extensor carpi radialis brevis, ECRL: m. extensor carpi radialis longus
Transverse ultrasound section of the dorsoradial portion of the wrist showing the second extensor compartment, located lateral to Lister's tubercle. In this view, the tendons of m. extensor carpi radialis brevis (ECRB) and m. extensor carpi radialis longus (ECRL) are visible, running close to the dorsal contour of the distal radius. This area is a common site of overuse and this view is important for evaluating tenosynovitis, irritative changes, and other pathological changes of the tendons of the second extensor compartment.
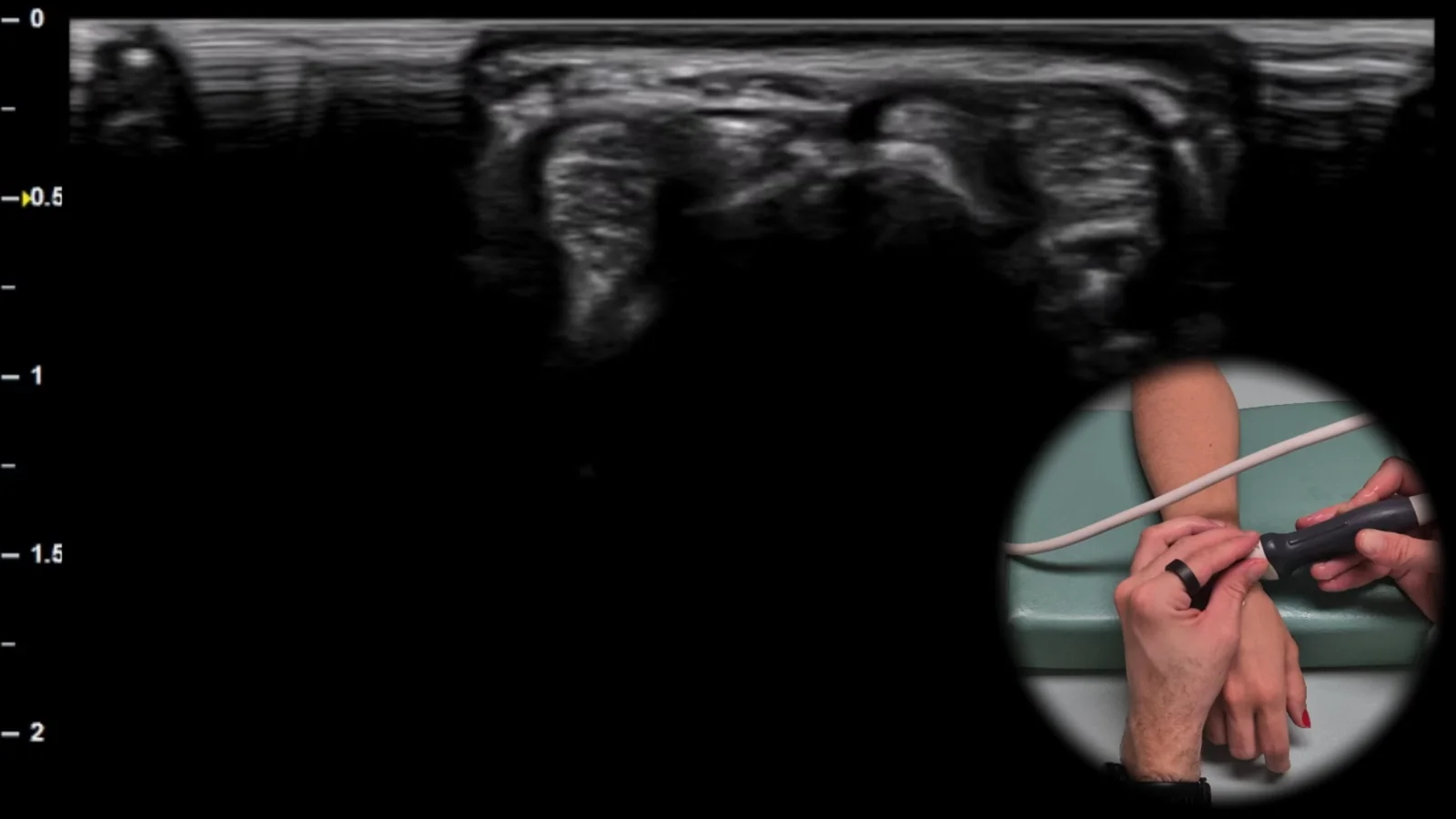
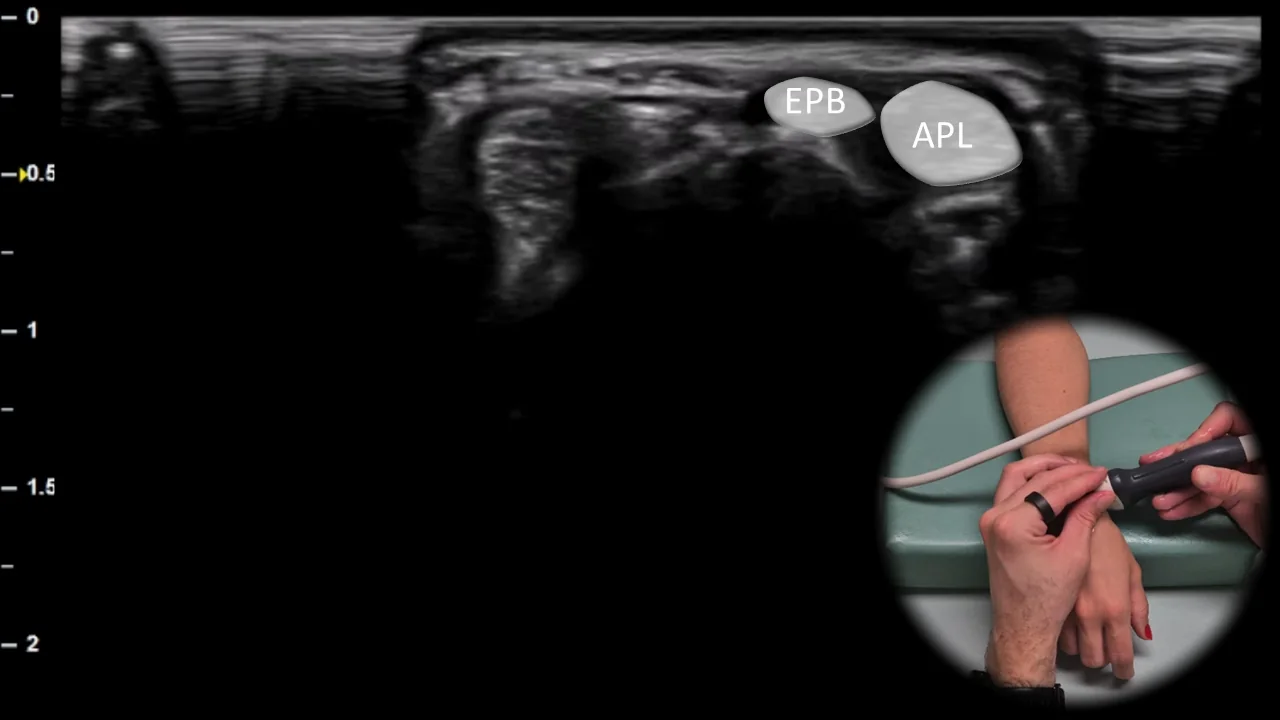
Figure 6. Dorsal view, transverse plane. EPB: m. extensor pollicis brevis, APL: m. abductor pollicis longus
Transverse ultrasound section of the dorsoradial part of the wrist showing the first extensor compartment. In this projection, the tendons of m. abductor pollicis longus (APL) and m. extensor pollicis brevis (EPB) are visible, running in a common tendon sheath over the radial styloid. This projection is typical for assessment of De Quervain's tenosynovitis and allows evaluation of sheath thickening, presence of fluid, and other signs of overuse in the first extensor compartment area.
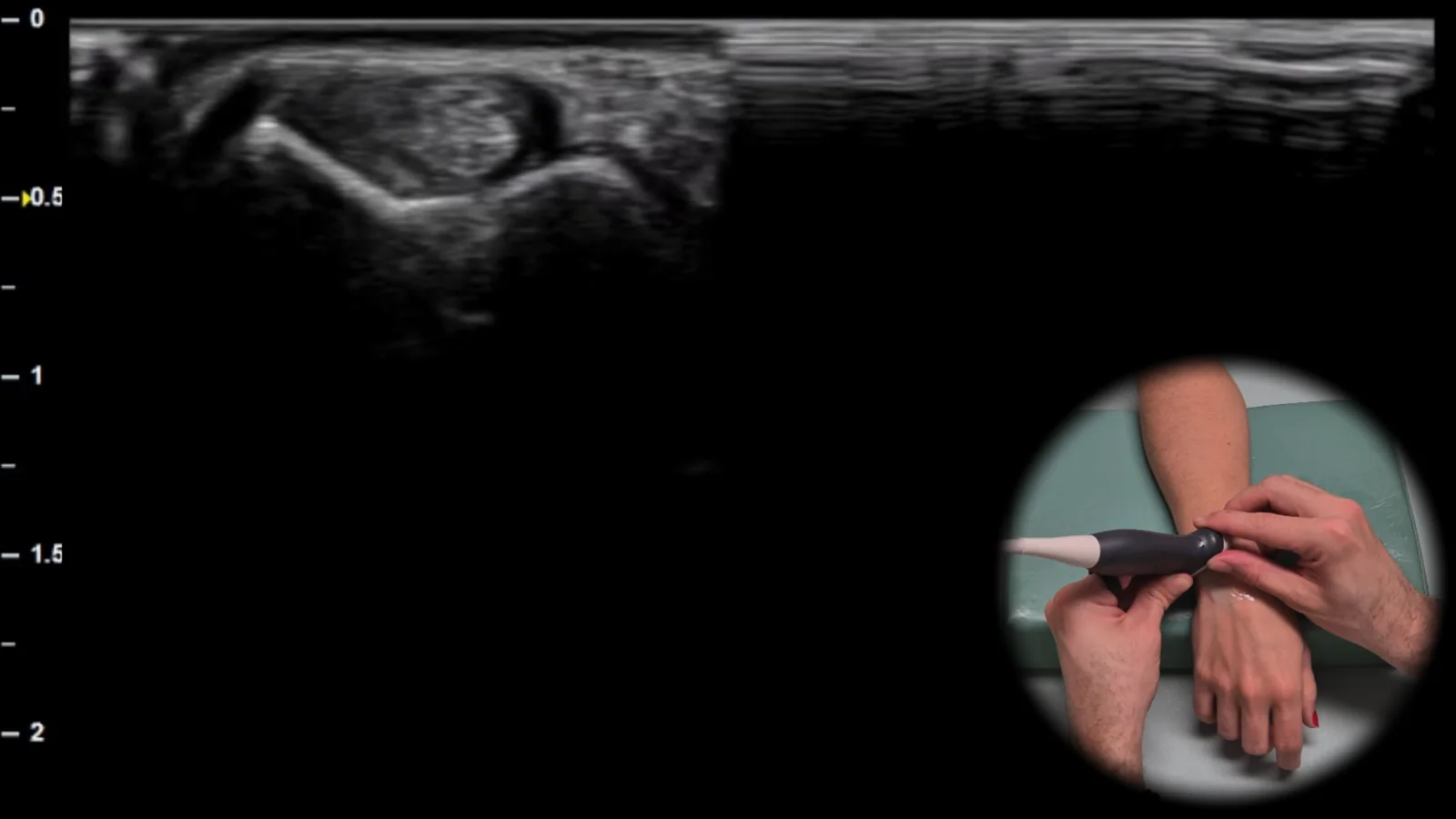
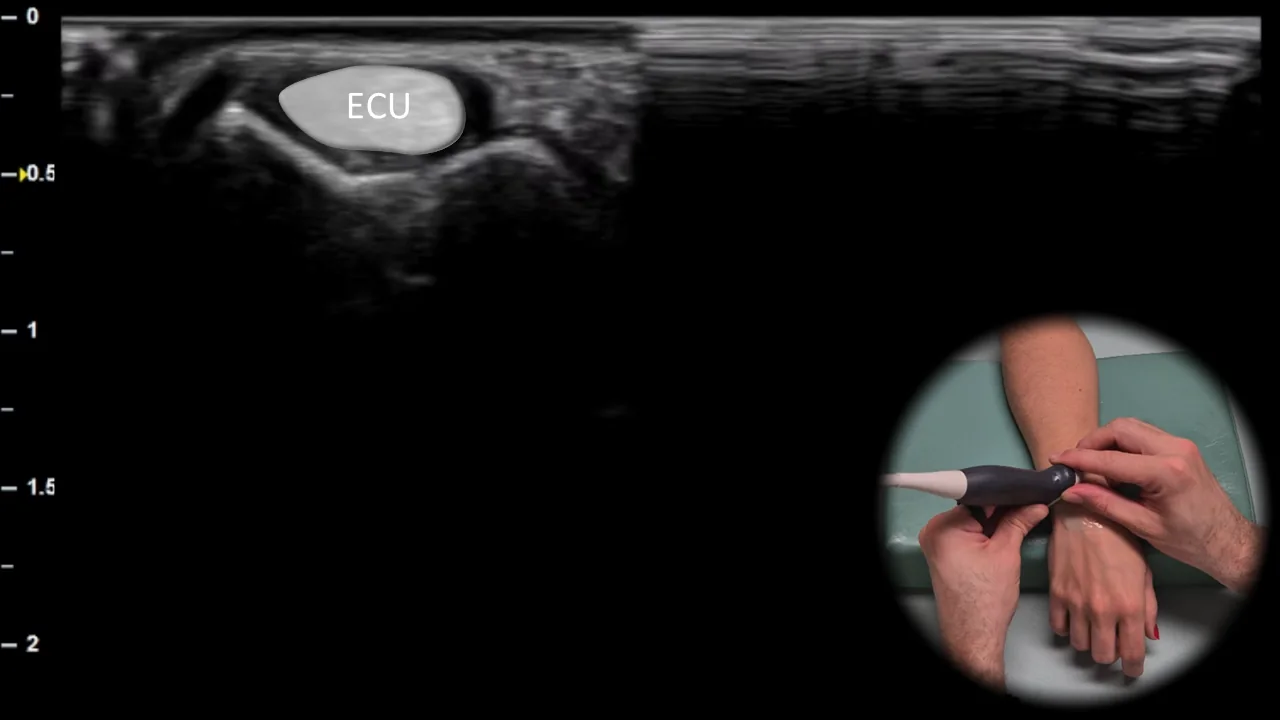
Figure 7. Dorsal view, transverse plane. ECU: m. extensor carpi ulnaris
Transverse ultrasound section of the dorsoulnar part of the wrist showing the sixth extensor compartment located over the ulna. In this projection, the extensor carpi ulnaris (ECU) tendon is visible, running in the ulnar groove as the main structure of this compartment. This projection is essential for evaluating tenosynovitis, instability and subluxation of the ECU tendon, especially during dynamic examination in connection with ulnar wrist pain.
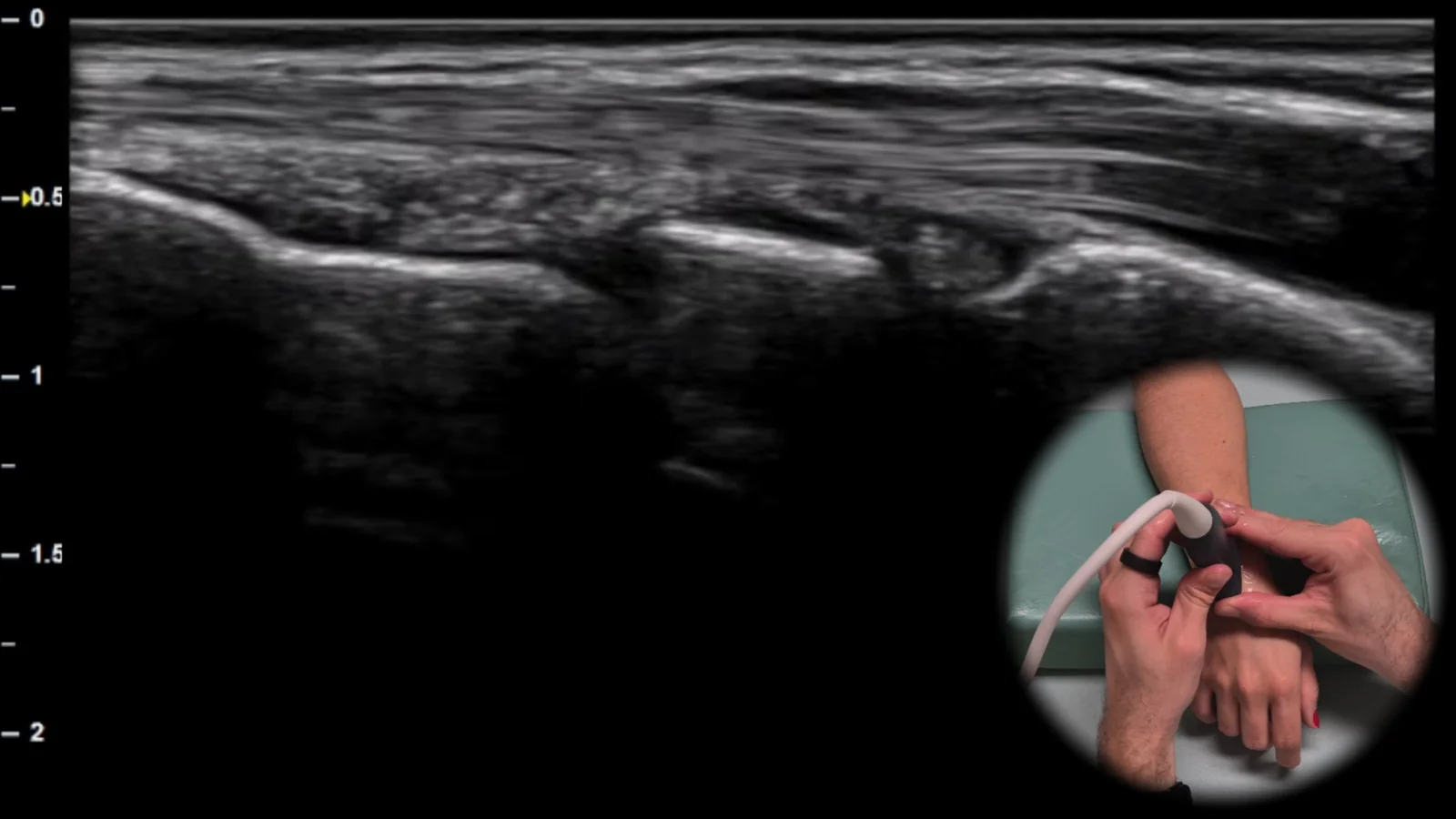
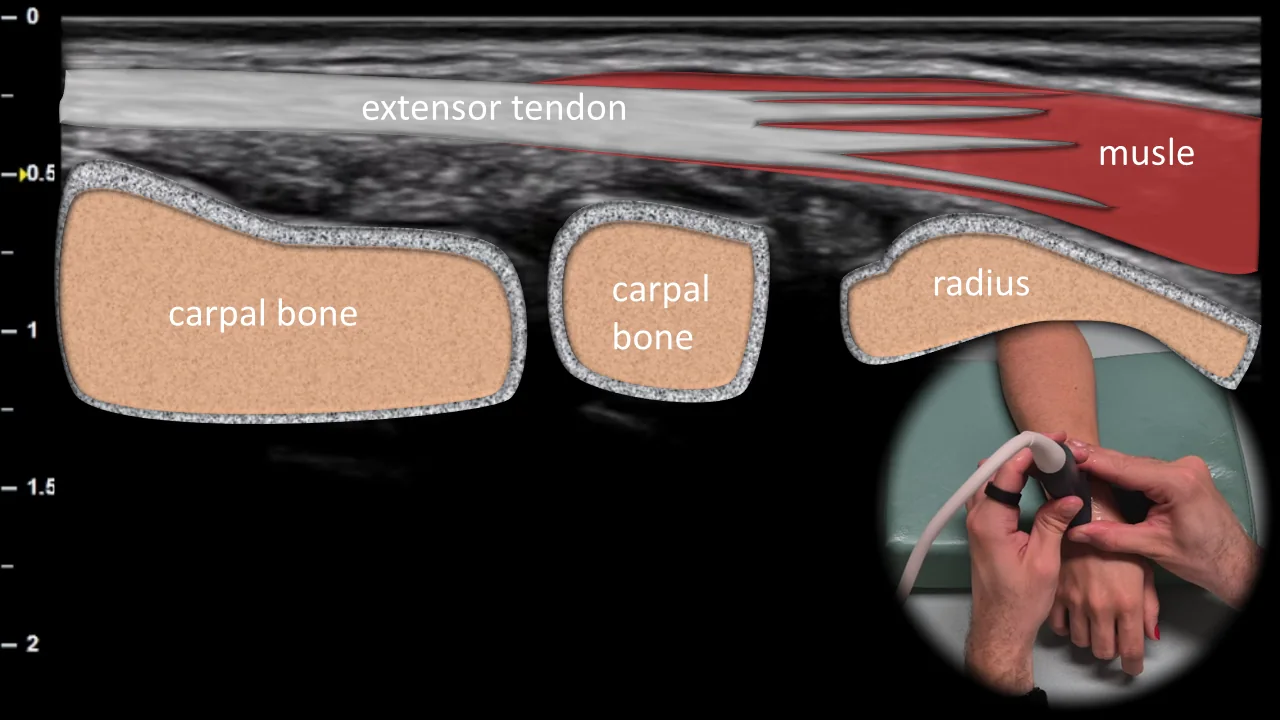
Figure 8. Dorsal view, sagittal plane.
Longitudinal ultrasound section of the dorsal side of the wrist showing extensor tendons in long axis above the radiocarpal joint. In this projection, extensor tendons are visible as fibrillar structures running superficially over the contour of the distal radius and carpal bones, with the imaging also including the radiocarpal joint area. This projection is important for detecting joint effusion, signs of synovitis, and for evaluating continuity of extensor tendons when partial or complete tendon injury is suspected.
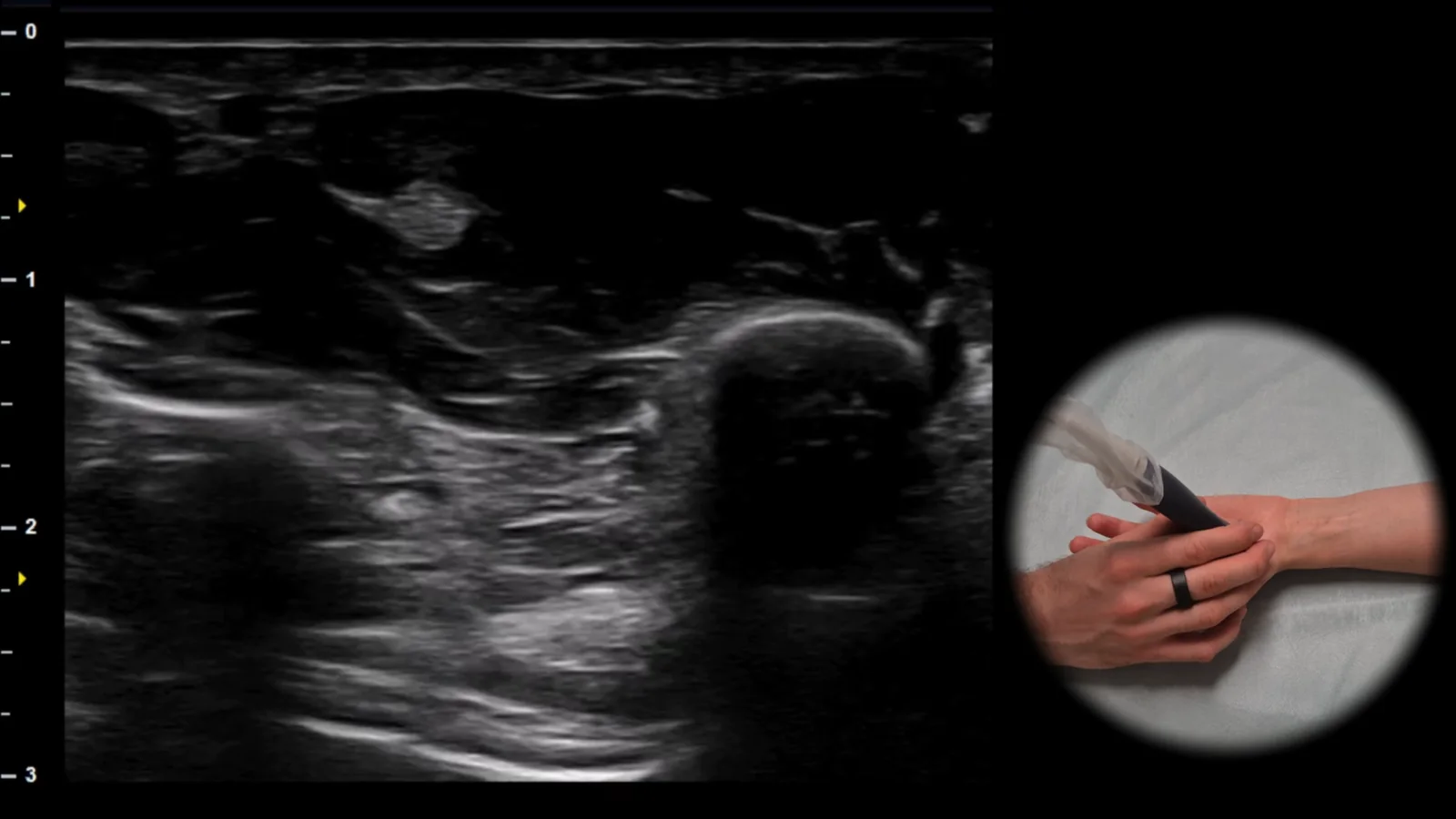
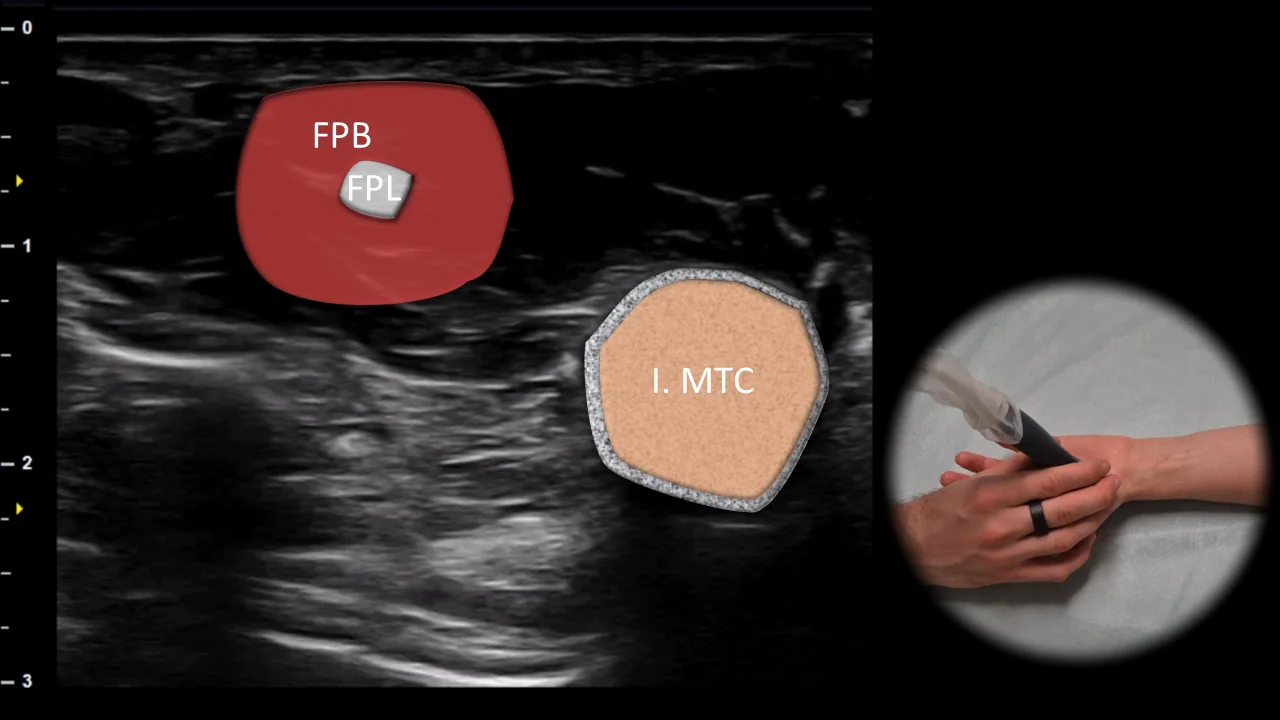
Figure 9. Thenar view, transverse plane. FPB: flexor pollicis brevis muscle, FPL: flexor pollicis longus tendon, I. MTC: first metacarpal
Transverse ultrasound section through the thenar region. The flexor pollicis brevis muscle (FPB) is visible superficially, with the flexor pollicis longus tendon (FPL) located within its muscle belly, appearing as a markedly hyperechoic oval structure. The bony interface of the first metacarpal (I. MTC) is visible laterally, serving as the main landmark for this projection. This projection allows clear visualization of the superficial soft tissue structures of the thenar and is useful in evaluating pathology of the FPL tendon and thumb muscles.
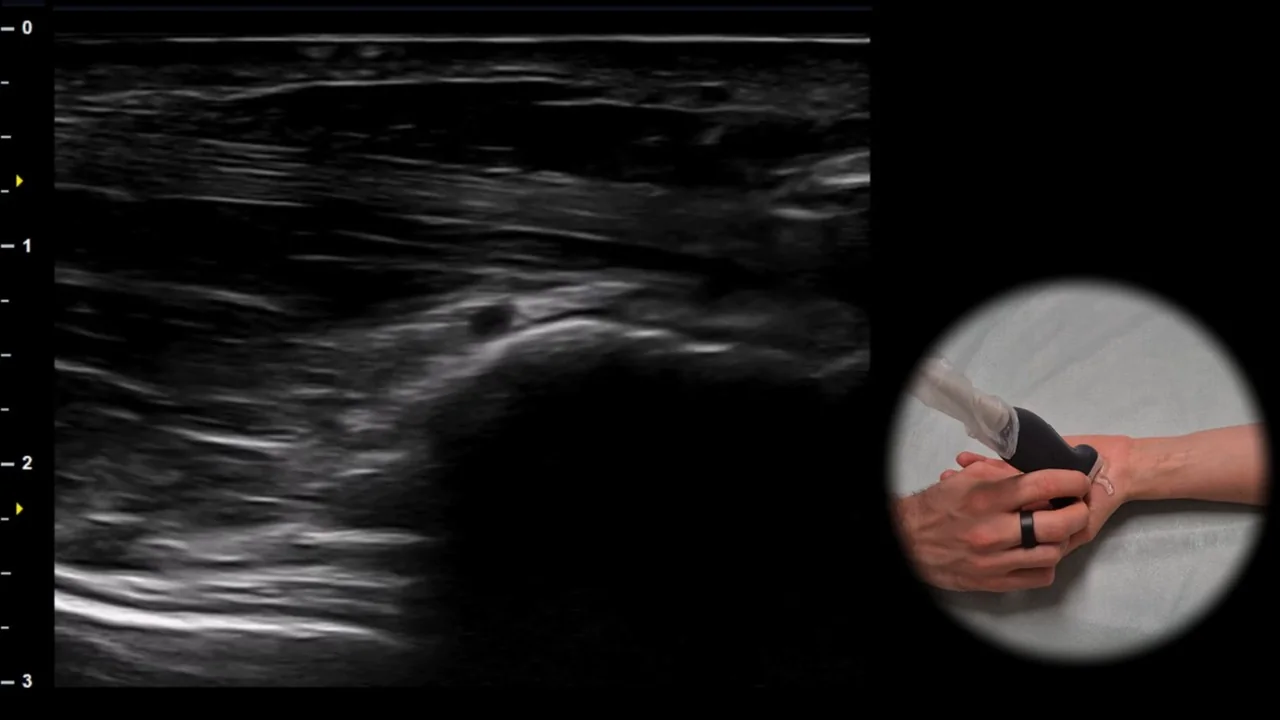
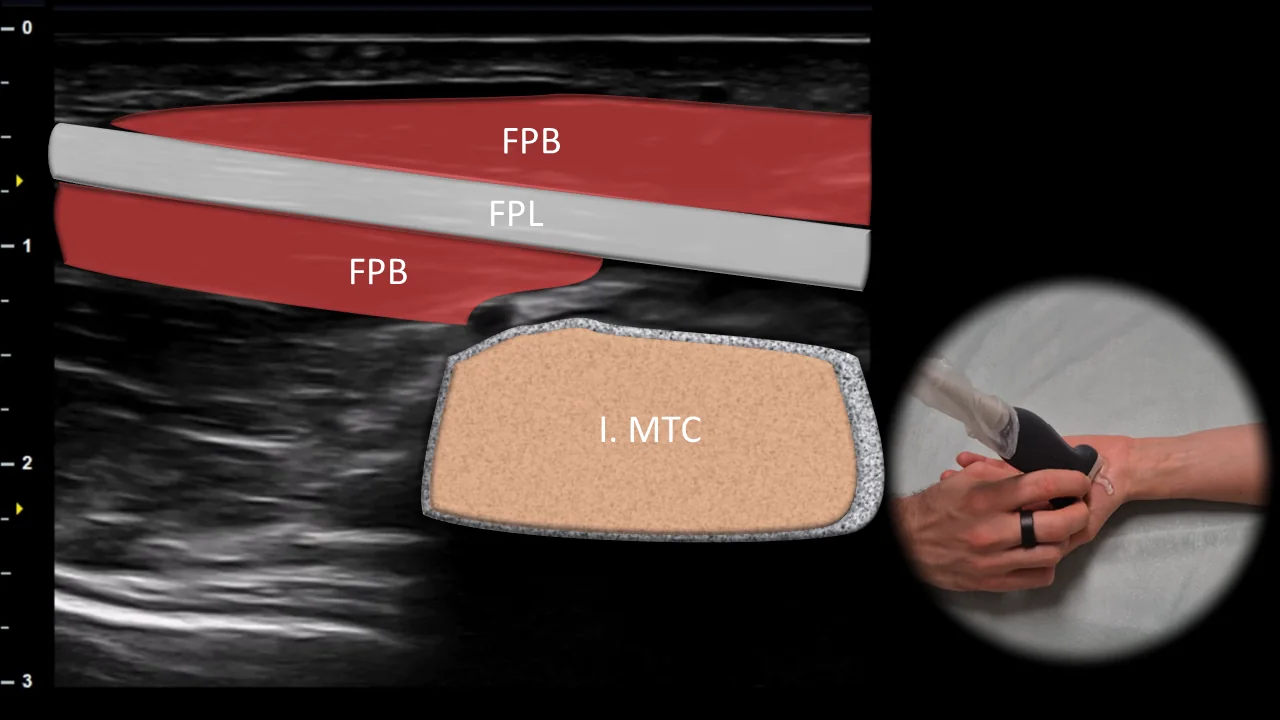
Figure 10. View of the thenar, sagittal plane. FPB: m. flexor pollicis brevis, FPL: tendon of m. flexor pollicis longus, I. MTC: first metacarpal
Longitudinal ultrasound section through the thenar region showing the m. flexor pollicis brevis (FPB) and the tendon of m. flexor pollicis longus (FPL) running along the first metacarpal (I. MTC). The FPL tendon is visible in this projection in long axis as a linear fibrillar structure located between the soft tissues of the thenar and the bony interface of the first metacarpal. This projection is suitable for dynamic examination of the FPL tendon during flexion in the interphalangeal joint of the thumb and allows assessment of its continuity, gliding, and any pathological changes.
4. View of the MCP Joint
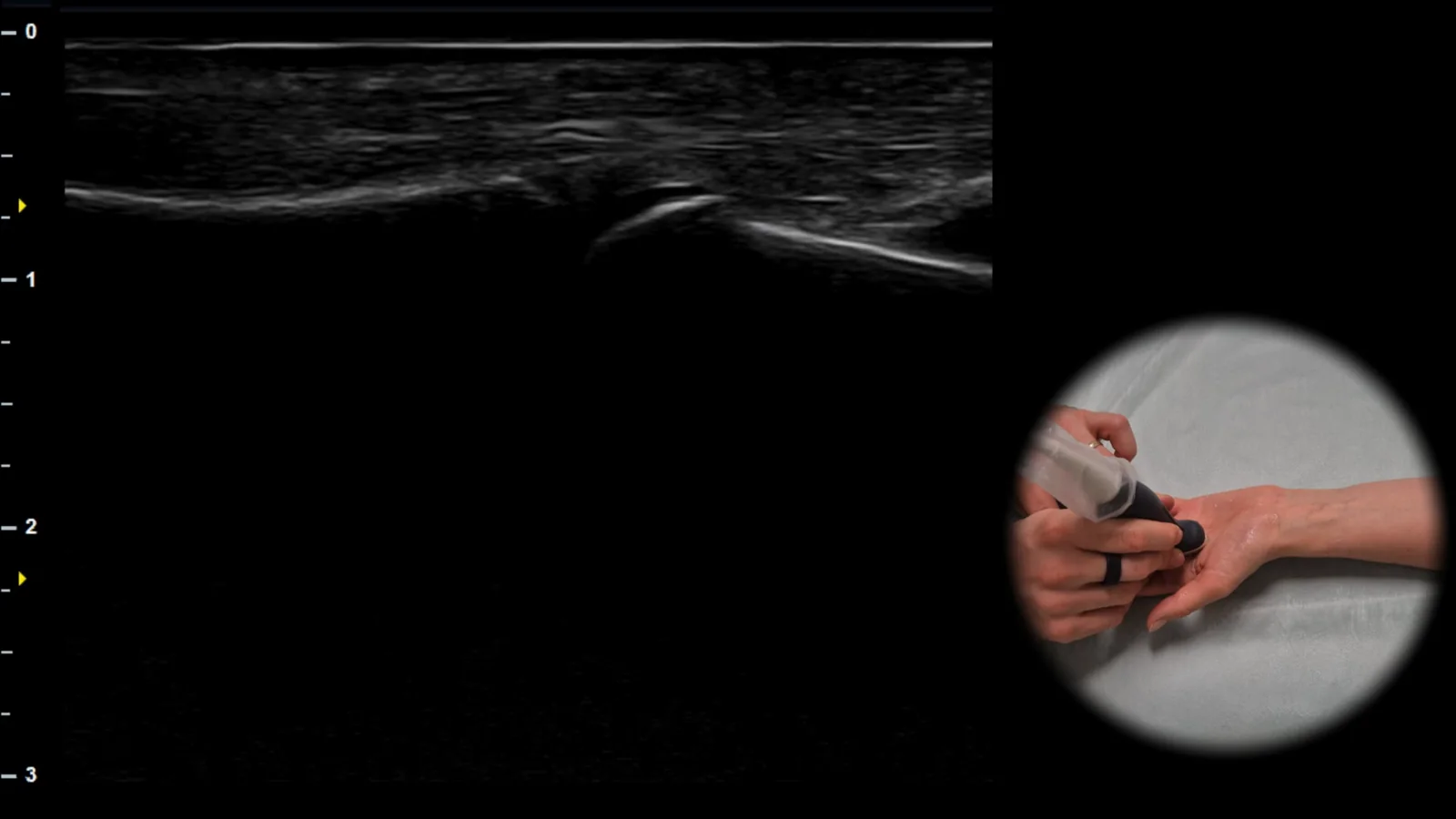
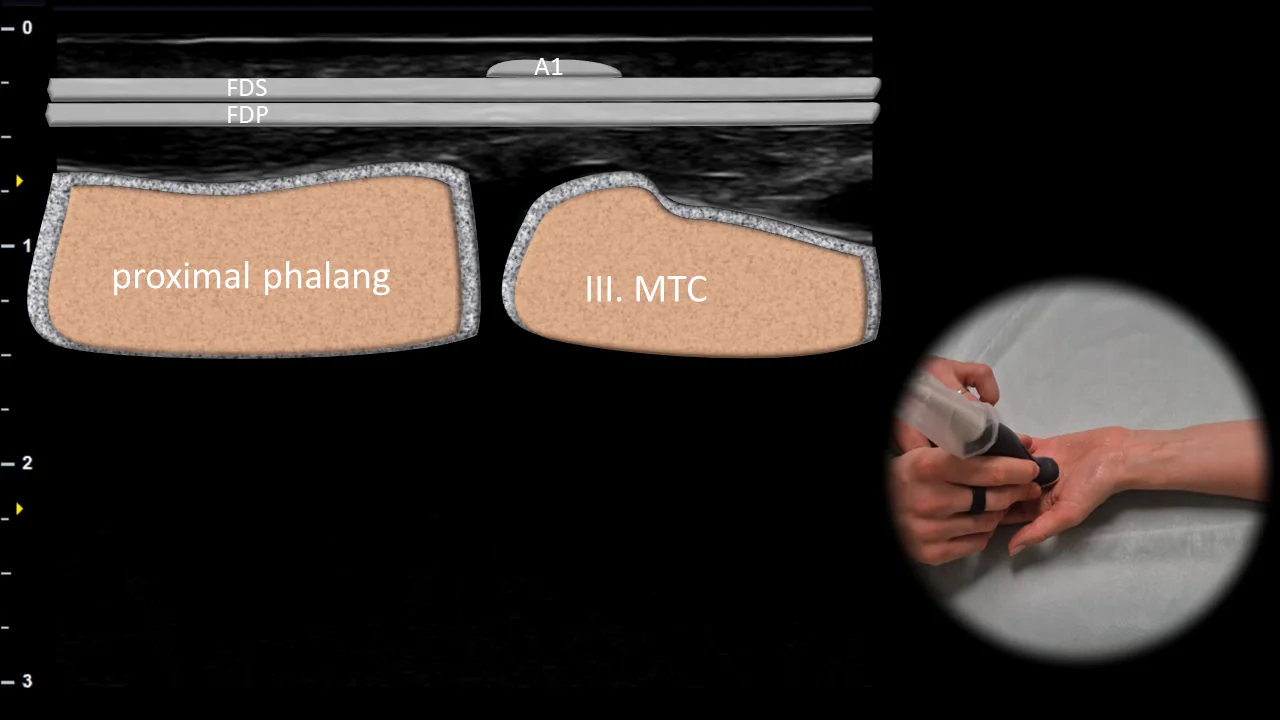
Figure 11. View of the MCP joint, sagittal plane. A1: A1 pulley, FDS: flexor digitorum superficialis tendon, FDP: flexor digitorum profundus tendon, III. MTC: third metacarpal
Longitudinal ultrasound section through the metacarpophalangeal joint region showing the finger flexor apparatus at the level of the A1 pulley. The A1 pulley is visible superficially above the flexor tendons, beneath which run the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons, while the head of the third metacarpal (III. MTC) serves as the bony landmark. This projection is important for evaluating the relationship of the flexor tendons to the A1 pulley and during dynamic examination allows assessment of their gliding, possible pulley thickening, and signs of stenosing tenosynovitis.
Unlock the full Health Library
Full access to scanning protocols, anatomy, and clinical references. Cancel anytime.
- Every protocol and anatomy reference
- Original ultrasound illustrations and video demonstrations
- Sync across mobile and web